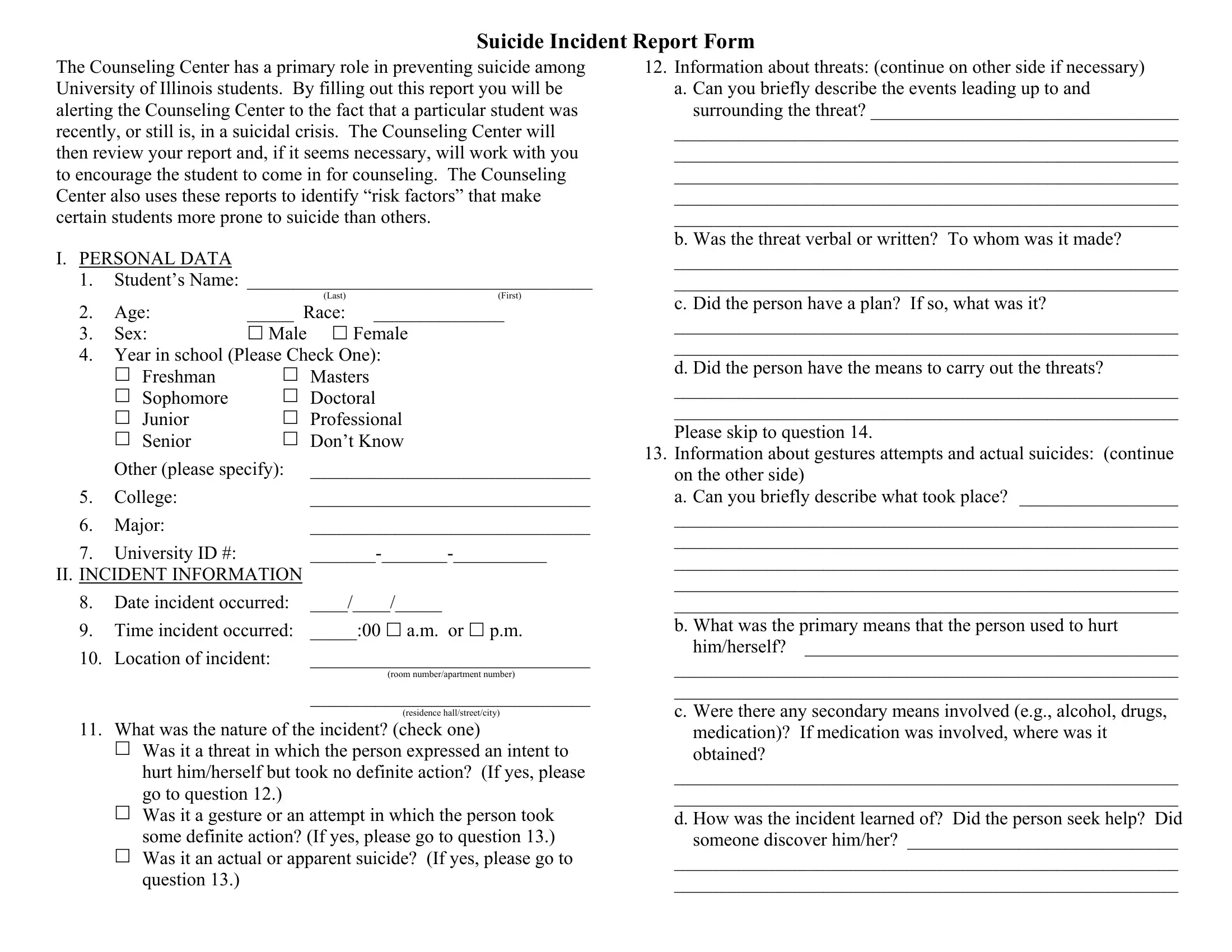
The Counseling Center has a primary role in preventing suicide among University of Illinois students. By filling out this report you will be alerting the Counseling Center to the fact that a particular student was recently, or still is, in a suicidal crisis. The Counseling Center will then review your report and, if it seems necessary, will work with you to encourage the student to come in for counseling. The Counseling Center also uses these reports to identify “risk factors” that make certain students more prone to suicide than others.
I.PERSONAL DATA
1. Student’s Name: _____________________________________
|
|
(Last) |
(First) |
2. |
Age: |
_____ Race: |
______________ |
3. |
Sex: |
Male |
Female |
4.Year in school (Please Check One):
|
Freshman |
Masters |
|
Sophomore |
Doctoral |
|
Junior |
Professional |
|
Senior |
Don’t Know |
|
Other (please specify): |
______________________________ |
5. |
College: |
______________________________ |
6. |
Major: |
______________________________ |
7. |
University ID #: |
_______-_______-__________ |
II.INCIDENT INFORMATION
8.Date incident occurred: ____/____/_____
9. |
Time incident occurred: |
_____:00 a.m. or p.m. |
10. |
Location of incident: |
______________________________ |
(room number/apartment number)
______________________________
(residence hall/street/city)
11. What was the nature of the incident? (check one)
Was it a threat in which the person expressed an intent to hurt him/herself but took no definite action? (If yes, please go to question 12.)
Was it a gesture or an attempt in which the person took some definite action? (If yes, please go to question 13.) Was it an actual or apparent suicide? (If yes, please go to question 13.)
12.Information about threats: (continue on other side if necessary)
a.Can you briefly describe the events leading up to and surrounding the threat? _________________________________
______________________________________________________
______________________________________________________
______________________________________________________
______________________________________________________
______________________________________________________
b. Was the threat verbal or written? To whom was it made?
______________________________________________________
______________________________________________________
c. Did the person have a plan? If so, what was it?
______________________________________________________
______________________________________________________
d. Did the person have the means to carry out the threats?
______________________________________________________
______________________________________________________
Please skip to question 14.
13.Information about gestures attempts and actual suicides: (continue on the other side)
a.Can you briefly describe what took place? _________________
______________________________________________________
______________________________________________________
______________________________________________________
______________________________________________________
______________________________________________________
b.What was the primary means that the person used to hurt
him/herself? ________________________________________
______________________________________________________
______________________________________________________
c. Were there any secondary means involved (e.g., alcohol, drugs, medication)? If medication was involved, where was it obtained?
______________________________________________________
______________________________________________________
d. How was the incident learned of? Did the person seek help? Did someone discover him/her? _____________________________
______________________________________________________
______________________________________________________