We have applied the efforts of the best software engineers to make the PDF editor you can benefit from. The app will let you fill out the tennessee first work document effortlessly and don’t waste time. Everything you need to undertake is adhere to the following simple instructions.
Step 1: The initial step would be to choose the orange "Get Form Now" button.
Step 2: You can now modify the tennessee first work. You need to use the multifunctional toolbar to add, delete, and change the text of the document.
Complete the tennessee first work PDF by entering the content needed for every single section.
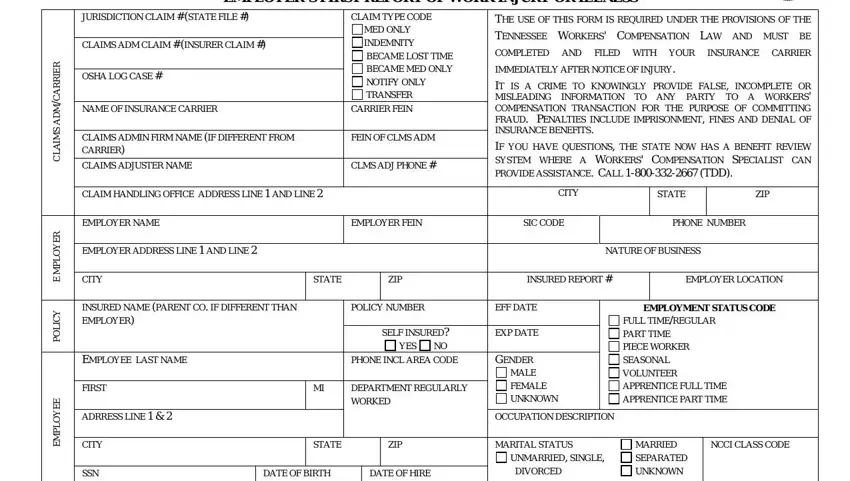
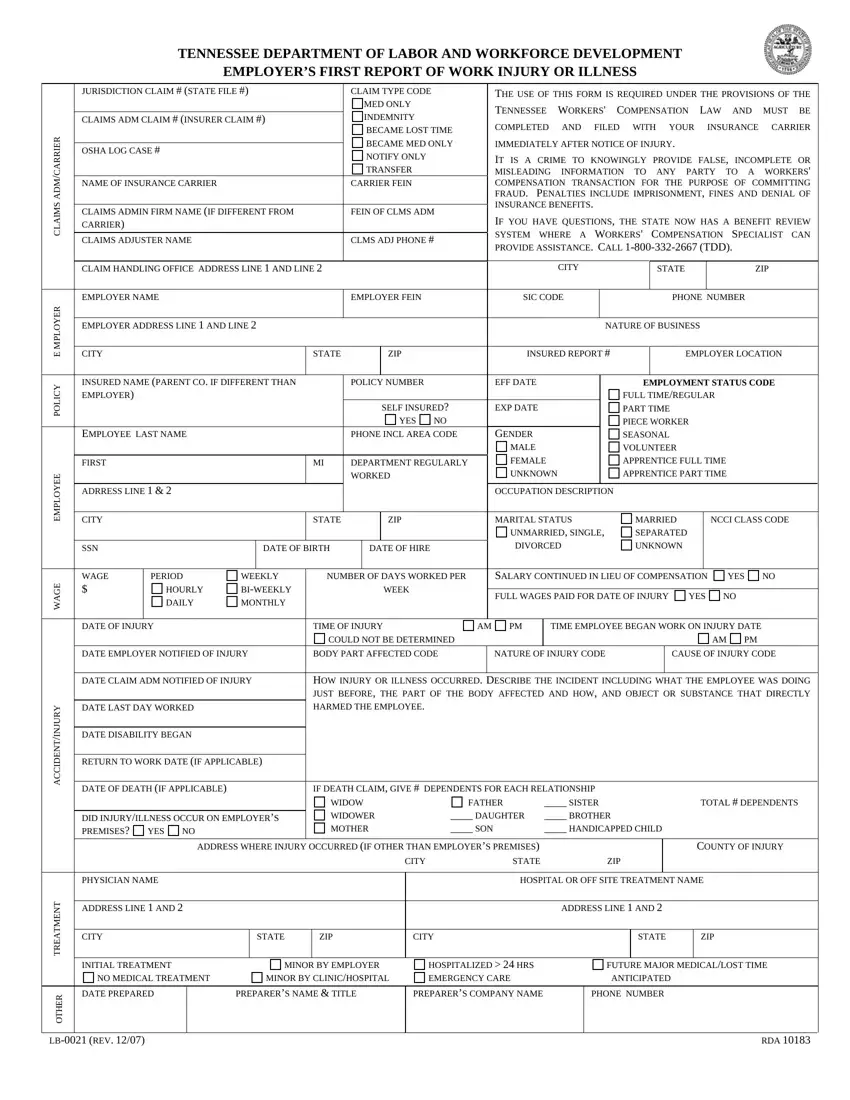
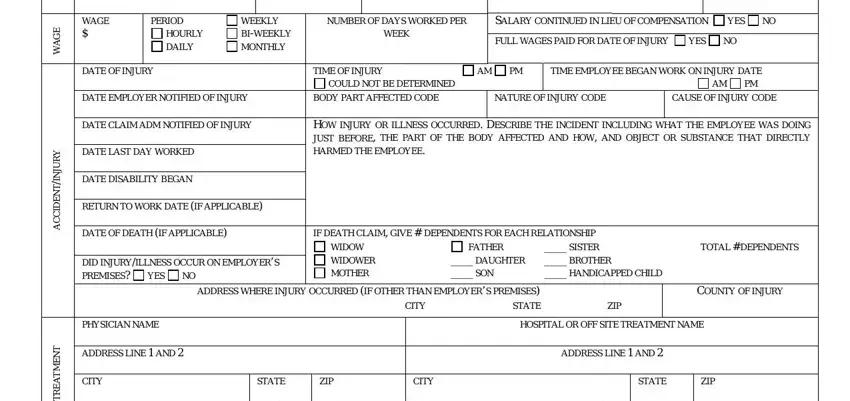
Write down the essential details in WAGE, PERIOD, HOURLY DAILY, WEEKLY BIWEEKLY MONTHLY, NUMBER OF DAYS WORKED PER WEEK, SALARY CONTINUED IN LIEU OF, YES, FULL WAGES PAID FOR DATE OF INJURY, YES, DATE OF INJURY, TIME OF INJURY COULD NOT BE, TIME EMPLOYEE BEGAN WORK ON INJURY, DATE EMPLOYER NOTIFIED OF INJURY, BODY PART AFFECTED CODE, and NATURE OF INJURY CODE area.
The software will request particulars to automatically prepare the section INITIAL TREATMENT, NO MEDICAL TREATMENT, MINOR BY EMPLOYER MINOR BY, HOSPITALIZED HRS EMERGENCY CARE, FUTURE MAJOR MEDICALLOST TIME, ANTICIPATED, T N E M T A E R T, DATE PREPARED R E H T O, LB REV, PREPARERS NAME TITLE, PREPARERS COMPANY NAME, PHONE NUMBER, and RDA.

Step 3: Choose the "Done" button. Now you may upload the PDF form to your electronic device. As well as that, you may send it through electronic mail.
Step 4: Generate copies of the file - it can help you stay away from potential future difficulties. And don't be concerned - we are not meant to disclose or check the information you have.
