
We were creating this PDF editor having the notion of allowing it to be as easy to apply as possible. That's the reason the actual procedure of creating the blue form will likely to be effortless perform all of these steps:
Step 1: Hit the "Get Form Now" button to start out.
Step 2: Now you should be within the document edit page. It's possible to add, alter, highlight, check, cross, include or delete areas or phrases.
Enter the information requested by the program to get the document.
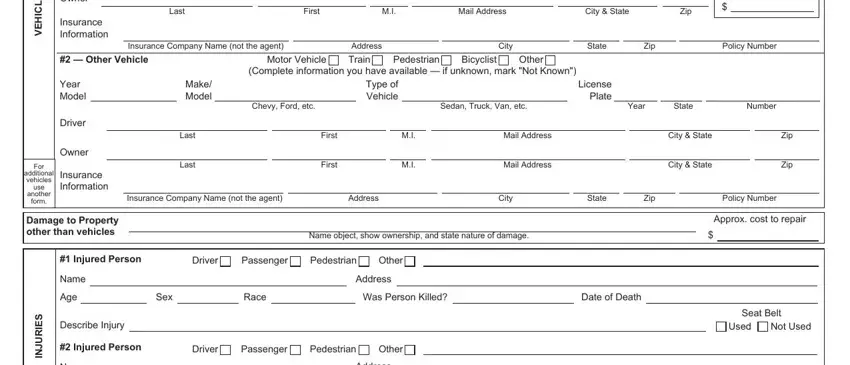
Within the part S E L C H E V, Owner, Insurance Information, Last, First, Mail Address, City State, Zip, Insurance Company Name not the, Address, City, State, Zip, Policy Number, and Other Vehicle write down the information which the software requests you to do.
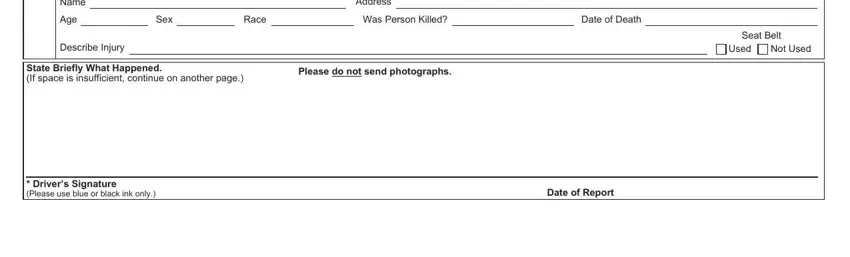
You could be requested for specific key particulars if you need to fill out the Name, Age, Describe Injury, Address, Sex, Race, Was Person Killed, Date of Death, State Briefly What Happened If, Please do not send photographs, Seat Belt, Used, Not Used, Drivers Signature Please use blue, and Date of Report field.
Step 3: Click the button "Done". Your PDF file can be transferred. You will be able download it to your device or send it by email.
Step 4: You can make duplicates of the document tokeep clear of all of the possible issues. Don't worry, we don't distribute or record your information.
