You'll find nothing difficult related to working with the report medical evaluation once you begin using our tool. By simply following these basic steps, you will receive the fully filled out file in the minimum time feasible.
Step 1: Select the orange "Get Form Now" button on the page.
Step 2: The document editing page is now available. Include information or change present information.
To obtain the form, enter the details the system will request you to for each of the next segments:
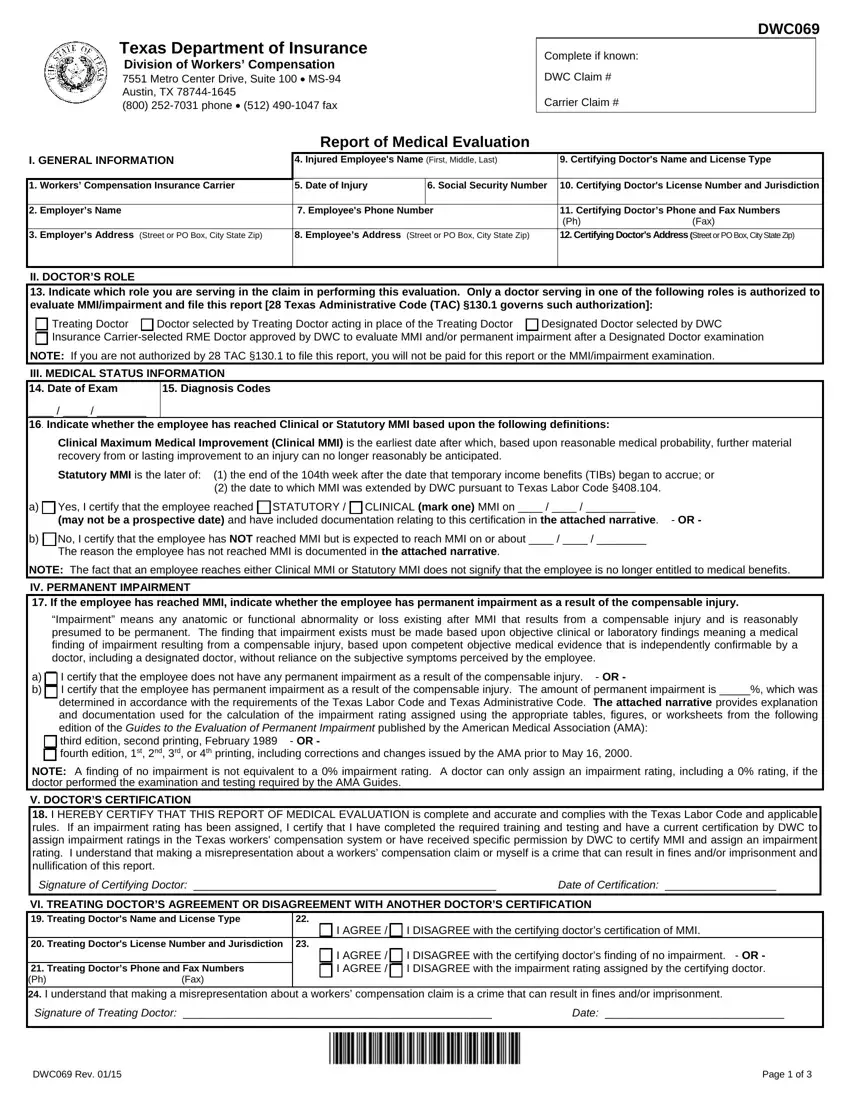
Type in the essential particulars in the area Yes I certify that the employee, No I certify that the employee has, NOTE The fact that an employee, IV PERMANENT IMPAIRMENT If the, Impairment means any anatomic or, a b, I certify that the employee does, NOTE A finding of no impairment is, V DOCTORS CERTIFICATION I HEREBY, and Signature of Certifying Doctor.
The software will request you to give certain essential details to conveniently fill out the part Signature of Certifying Doctor, I AGREE, I DISAGREE with the certifying, Treating Doctors License Number, Treating Doctors Phone and Fax, I AGREE I AGREE, I DISAGREE with the certifying, Signature of Treating Doctor Date, and DWC Rev Page of.
Step 3: Click the Done button to save the document. Now it is readily available for transfer to your electronic device.
Step 4: It will be easier to create copies of your document. There is no doubt that we are not going to disclose or see your details.
