
In case you need to fill out caregiver timesheet template, there's no need to install any sort of applications - just use our online tool. Our tool is consistently evolving to give the best user experience achievable, and that's because of our dedication to continuous development and listening closely to customer comments. To get the ball rolling, consider these easy steps:
Step 1: Press the "Get Form" button in the top section of this webpage to access our PDF editor.
Step 2: Once you launch the online editor, you will get the document made ready to be filled in. Other than filling in different blank fields, you might also do various other things with the file, particularly adding your own text, editing the original textual content, inserting images, placing your signature to the PDF, and more.
Completing this form calls for attention to detail. Make sure that all mandatory areas are filled in properly.
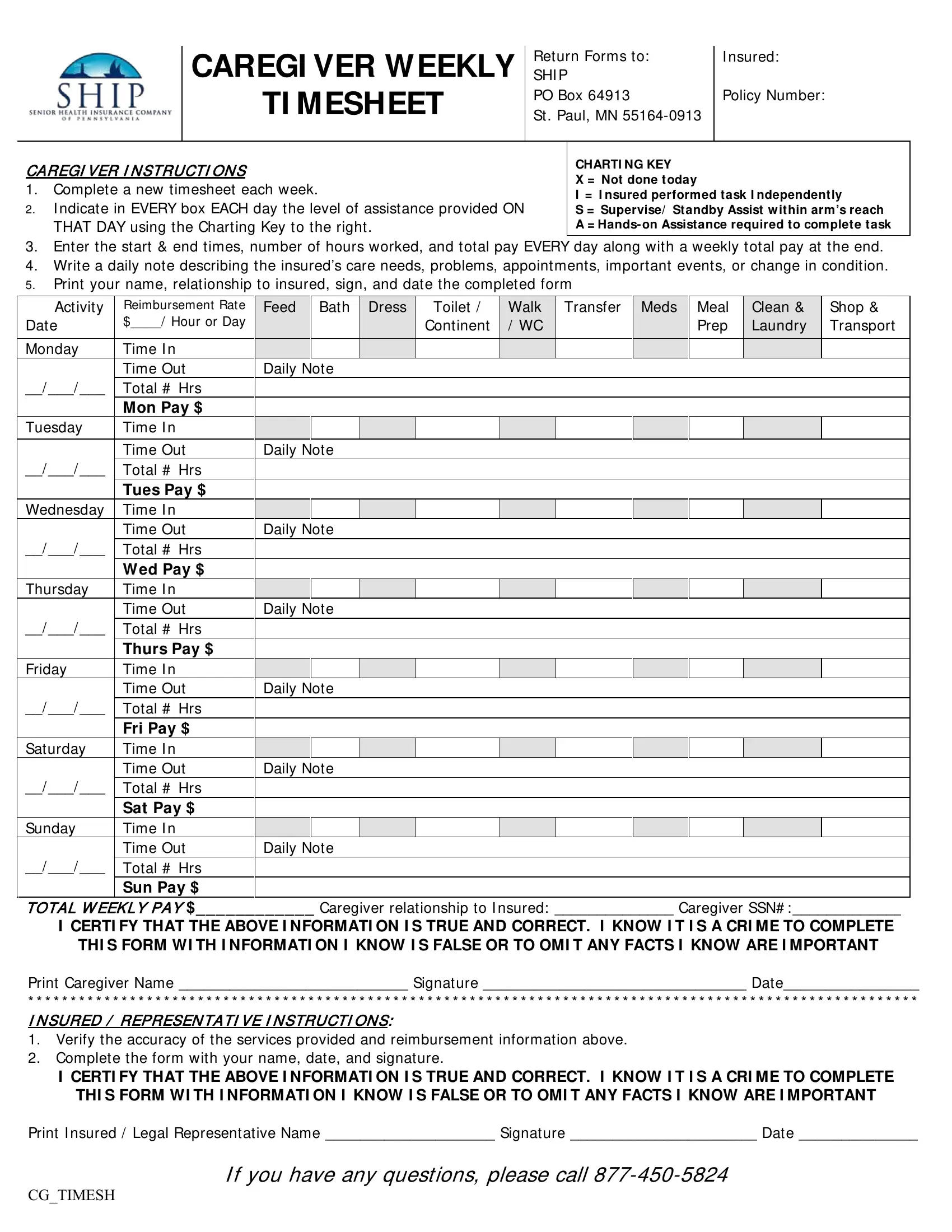
1. Complete the caregiver timesheet template with a number of essential blank fields. Get all of the required information and make sure not a single thing overlooked!
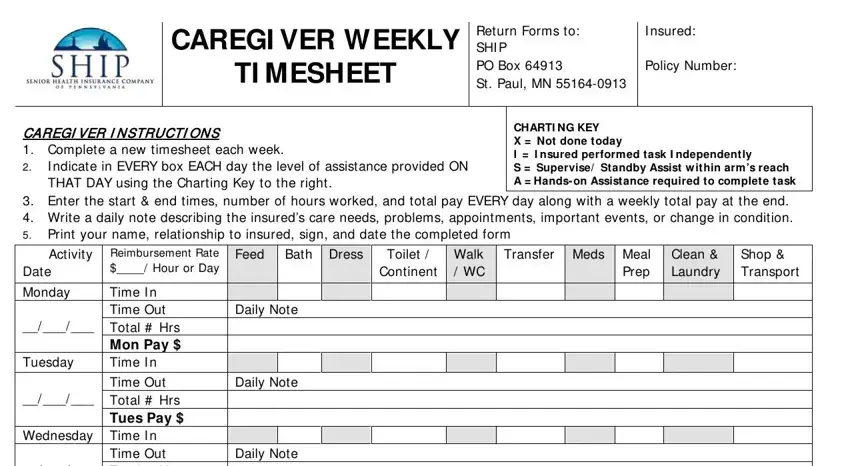
2. Now that the previous section is done, you should add the essential particulars in Thursday, Friday, Saturday, Sunday, Time Out Total Hrs Wed Pay Time, Wednesday Time I n, Daily Note Daily Note Daily Note, TOTAL WEEKLY PAY Caregiver, THI S FORM WI TH I NFORMATI ON I, and Print Caregiver Name Signature allowing you to progress to the 3rd part.
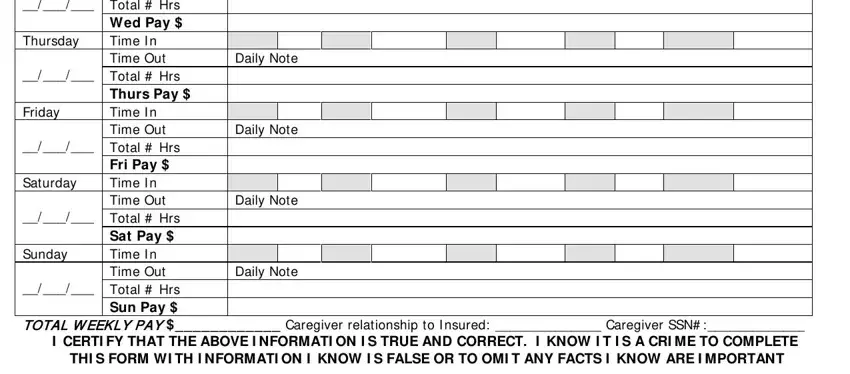
Regarding Print Caregiver Name Signature and TOTAL WEEKLY PAY Caregiver, make certain you take a second look here. Both these are certainly the most important ones in this document.
3. The following part is all about Print Caregiver Name Signature, I CERTI FY THAT THE ABOVE I, THI S FORM WI TH I NFORMATI ON I, Print I nsured Legal, If you have any questions please, and CGTIMESH - complete all of these fields.
Step 3: Reread all the information you have entered into the form fields and then click on the "Done" button. Create a 7-day free trial subscription with us and gain immediate access to caregiver timesheet template - download, email, or change inside your FormsPal account page. FormsPal is devoted to the personal privacy of all our users; we make certain that all personal information going through our editor stays secure.