

TLR can be filled out online easily. Simply open FormsPal PDF tool to get the job done without delay. Our editor is continually evolving to deliver the very best user experience attainable, and that's thanks to our resolve for constant improvement and listening closely to user feedback. With just several easy steps, you'll be able to begin your PDF journey:
Step 1: Press the "Get Form" button above. It is going to open up our tool so that you could start completing your form.
Step 2: As you launch the online editor, you will see the document prepared to be filled out. Besides filling in various fields, you could also perform many other actions with the PDF, such as putting on custom textual content, modifying the original text, inserting graphics, placing your signature to the document, and more.
So as to complete this document, be certain to type in the necessary information in each and every field:
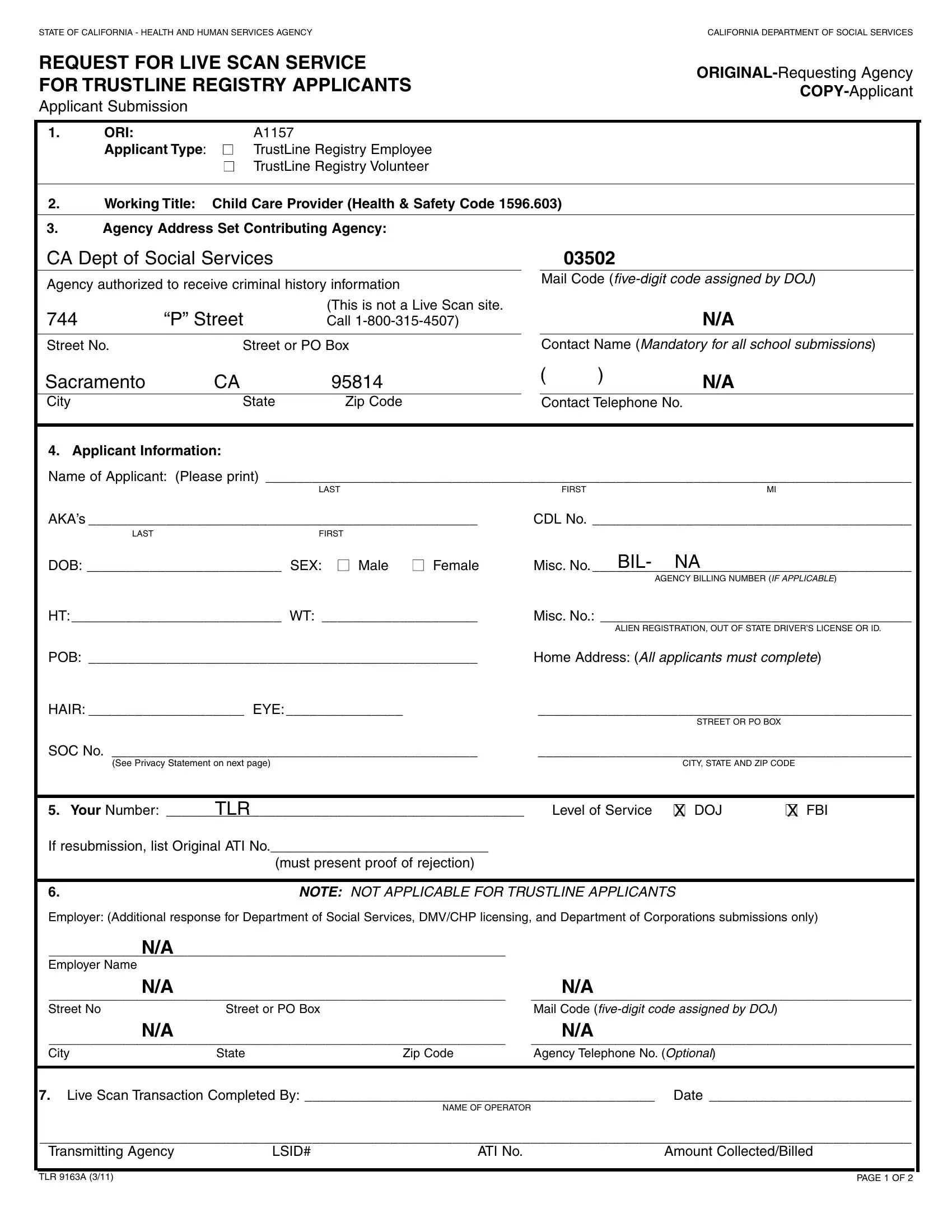
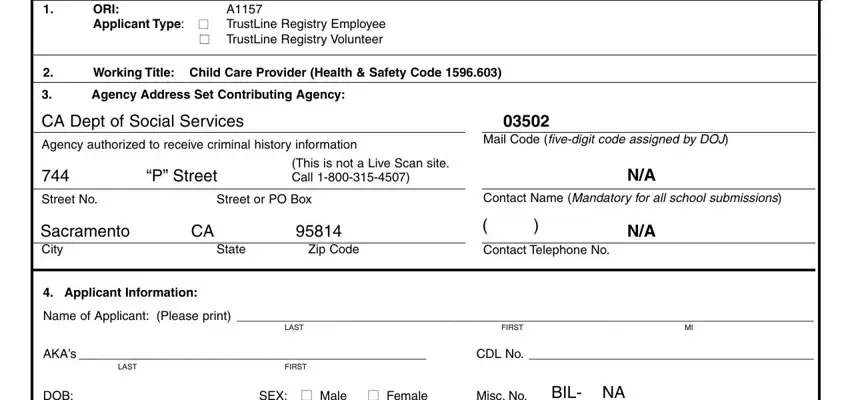
1. You need to complete the TLR properly, so be careful while working with the parts containing these blank fields:
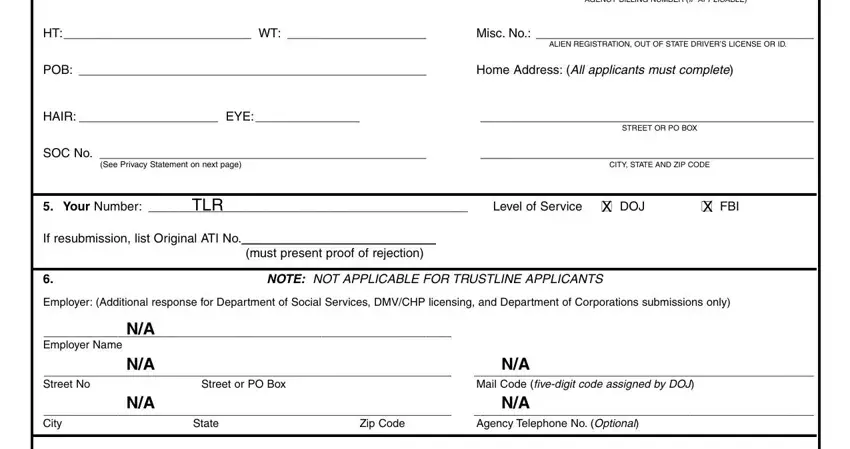
2. Once your current task is complete, take the next step – fill out all of these fields - AGENCY BILLING NUMBER IF APPLICABLE, HT WT, Misc No, ALIEN REGISTRATION OUT OF STATE, POB, Home Address All applicants must, HAIR EYE, STREET OR PO BOX, SOC No, See Privacy Statement on next page, CITY STATE AND ZIP CODE, Your Number, TLR, Level of Service DOJ, and X FBI with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
Be very careful while filling out STREET OR PO BOX and HT WT, since this is where most people make a few mistakes.
3. In this particular stage, look at Live Scan Transaction Completed, NAME OF OPERATOR, Transmitting Agency, LSID, ATI No, Amount CollectedBilled, TLR A, and PAGE OF. These are required to be completed with greatest accuracy.

Step 3: Go through the details you have entered into the blank fields and click the "Done" button. Create a 7-day free trial account with us and get instant access to TLR - download or modify inside your personal account page. We don't share or sell the details that you type in whenever dealing with forms at our site.