Submitting files with our PDF editor is more straightforward than nearly anything. To enhance mtm online access the form, there's nothing you have to do - basically continue with the steps down below:
Step 1: Click on the "Get Form Here" button.
Step 2: After you've accessed the mtm online access edit page, you will notice all actions you may take with regards to your document within the upper menu.
You should provide the next details to create the mtm online access PDF:
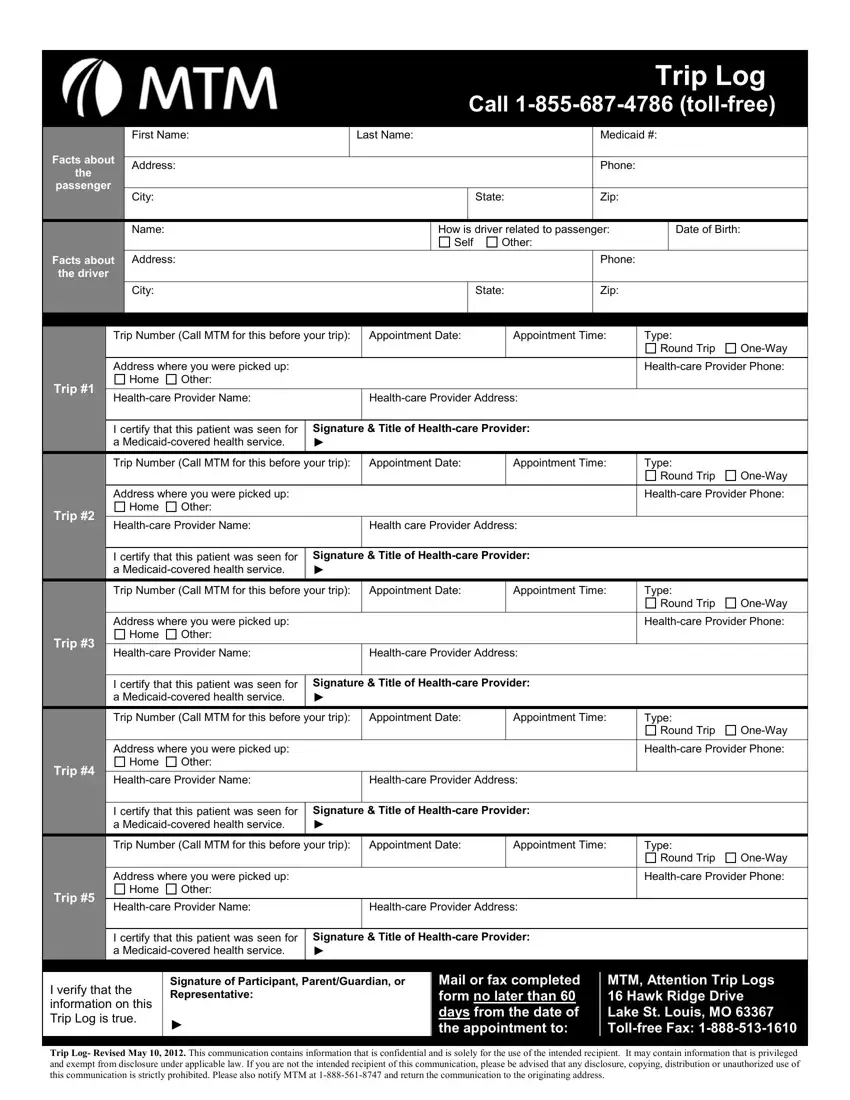
Put the essential particulars in the Trip, Trip, Trip, Trip Number Call MTM for this, Appointment Date, Appointment Time, Type, Address where you were picked up, Home, Other, Round Trip, OneWay, Healthcare Provider Phone, Healthcare Provider Name, and Healthcare Provider Address field.
Provide the key data the I verify that the information on, Signature of Participant, Mail or fax completed form no, MTM Attention Trip Logs Hawk, and Trip Log Revised May This part.

The area Trip, Trip, Trip, Trip, Trip Number Call MTM for this, Appointment Date, Appointment Time, Type, Address where you were picked up, Home, Other, Round Trip, OneWay, Healthcare Provider Phone, and Healthcare Provider Name is going to be where one can insert both sides' rights and obligations.
Finish by reviewing the following sections and filling them out correspondingly: Trip, Trip, Trip, I certify that this patient was, Signature Title of Healthcare, Trip Number Call MTM for this, Appointment Date, Appointment Time, Type, Address where you were picked up, Home, Other, Round Trip, OneWay, and Healthcare Provider Phone.
Step 3: Choose the button "Done". The PDF file can be transferred. You may upload it to your pc or send it by email.
Step 4: You will need to create as many copies of your form as possible to remain away from future misunderstandings.
