

Working with PDF files online is always easy using our PDF editor. You can fill out triwest secondary authorization request form here effortlessly. We are aimed at providing you the best possible experience with our tool by constantly introducing new capabilities and enhancements. With these updates, working with our editor gets easier than ever before! Getting underway is effortless! What you need to do is adhere to these simple steps below:
Step 1: Click on the "Get Form" button above. It is going to open our tool so that you could begin filling in your form.
Step 2: With this online PDF tool, it is possible to do more than merely fill in forms. Try all the functions and make your forms look perfect with customized textual content put in, or optimize the original input to perfection - all that supported by the capability to insert your own graphics and sign the document off.
This form will need you to enter specific information; in order to guarantee accuracy, you should adhere to the guidelines directly below:
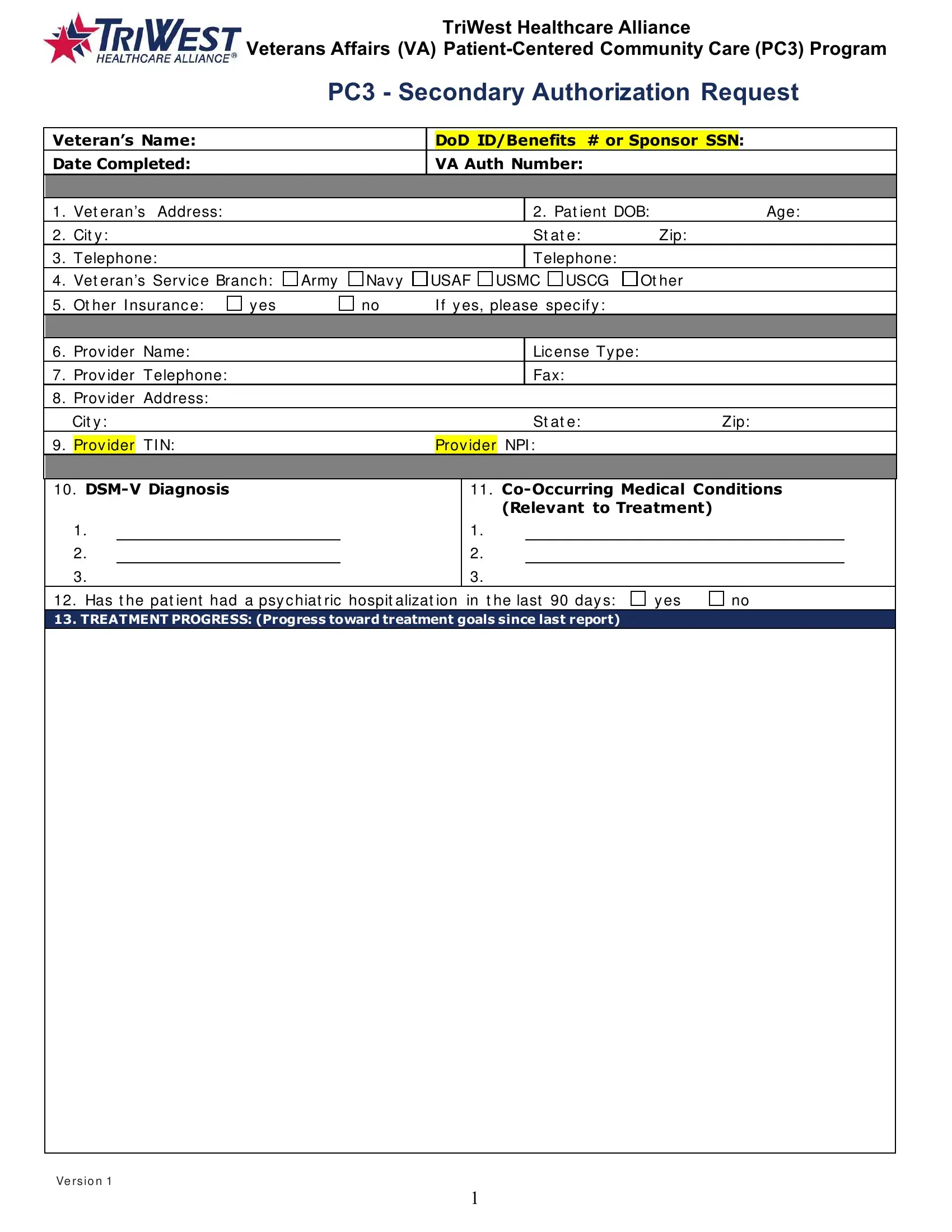
1. When filling in the triwest secondary authorization request form, make sure to incorporate all of the essential blank fields within the associated form section. It will help speed up the process, which allows your information to be handled fast and appropriately.
2. Right after completing this part, go on to the subsequent stage and fill in the necessary particulars in these blanks - Has t he pat ient had a psy c, and y es.
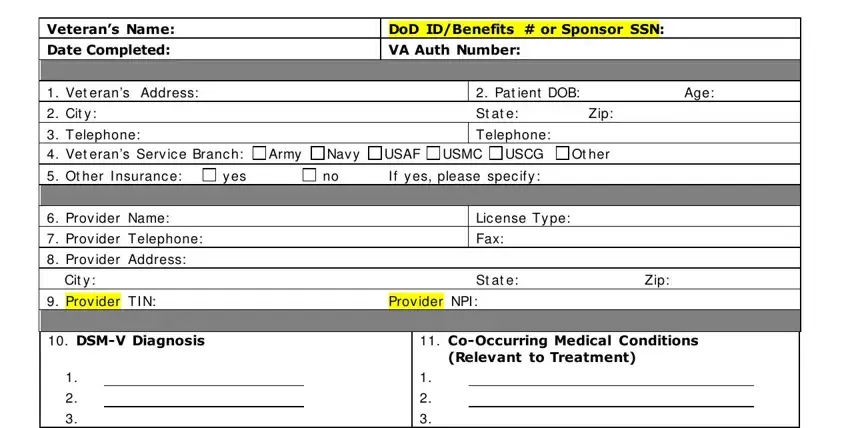
3. The following part will be focused on Veterans Name Date Completed, DoD IDBenefits or Sponsor SSN VA, TREATMENT PLAN UPDATE Please, Goals, and Methods - complete every one of these fields.
It is easy to make a mistake when filling out your Goals, for that reason make sure to reread it before you'll finalize the form.
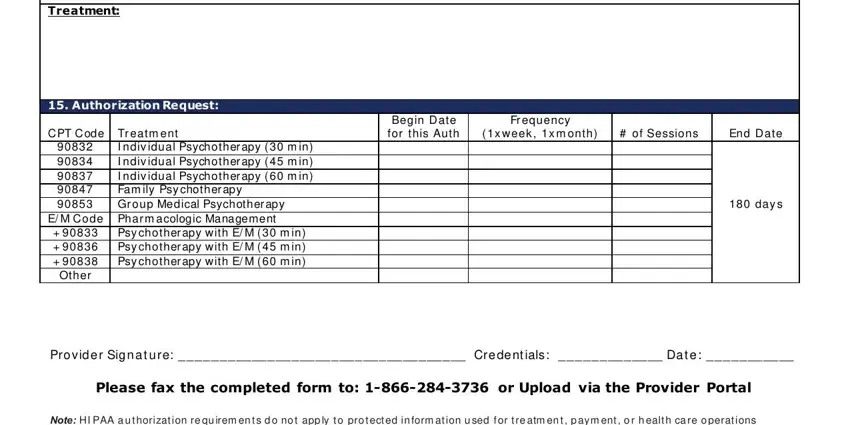
4. The subsequent paragraph requires your attention in the following places: Treatment, Authorization Request, C PT C ode Tr eatm ent, I ndiv idual Psychother apy m in, E M C ode Phar m acologic, Psy chother apy w ith E M m in, Begin D ate for this Auth, Fr equency, x w eek x m onth, of Sessions, End D ate, day s, Pro vid e r Sig n a t u re, Please fax the completed form to, and Note HI PAA a u t horizat ion re. Just remember to give all requested information to go further.
Step 3: Confirm that the details are accurate and then click "Done" to finish the project. Sign up with FormsPal now and immediately obtain triwest secondary authorization request form, ready for download. Each and every modification you make is handily kept , letting you customize the pdf further as required. When using FormsPal, you can easily complete documents without being concerned about information incidents or records getting shared. Our secure software helps to ensure that your private information is maintained safely.