With the purpose of making it as simple to use as it can be, we made the PDF editor. The process of filling up the trustmark claim form is going to be quick when you consider the next steps.
Step 1: To get started, click the orange button "Get Form Now".
Step 2: You can find all of the options which you can use on your document after you have accessed the trustmark claim form editing page.
Please enter the following information to complete the trustmark claim form PDF:
Provide the necessary data in the field Is accident a result of a Motor, Did the accident occur while on, Date of Initial Treatment, Where Treatment Received, Urgent Care Emergency Room ER, Date of FollowUp Visit, Where FollowUp Treatment Received, Urgent Care Emergency Room ER, and A Accident Claim Form V.
Indicate the essential data in Dates, Type of Room, Regular ICU Observation Unit, Admission Time Discharge Time, Please list all additional dates, Dates, Type of Room, Dates, Type of Room, Regular ICU Observation Unit, Regular ICU Observation Unit, Regular ICU Observation Unit, Regular ICU Observation Unit, Physical Therapy Please complete, and Date of initial physical therapy section.
In the section Fracture or Dislocation Please, Bones, Was surgery required Yes No Date, Was anesthesia required Yes No, Surgery When a Covered Person, Date of Surgery, Description of Surgery, Name of Facility where surgery was, Address of Facility, and A Accident Claim Form V, place the rights and responsibilities of the parties.
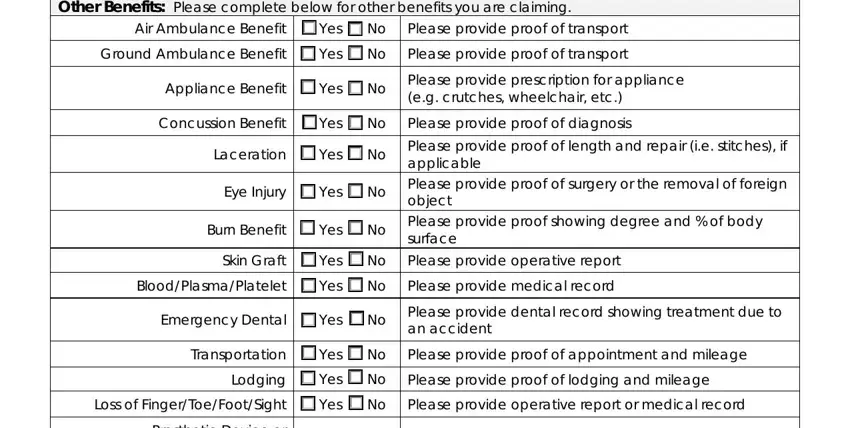
Finish by reviewing the following areas and filling them out as needed: Other Benefits Please complete, Air Ambulance Benefit Yes No, Please provide proof of transport, Please provide proof of transport, Appliance Benefit Yes No, Please provide prescription for, Concussion Benefit Yes No, Please provide proof of diagnosis, Laceration Yes No, Eye Injury Yes No, Burn Benefit Yes No, Please provide proof of length and, Skin Graft Yes No, Please provide operative report, and Please provide medical record.
Step 3: As soon as you select the Done button, your prepared file can be easily transferred to any of your gadgets or to email chosen by you.
Step 4: Make at least several copies of your form to stay away from any sort of potential future problems.
