The trustmark accident claim form filling out procedure is quick. Our PDF tool enables you to work with any PDF document.
Step 1: The following webpage contains an orange button saying "Get Form Now". Simply click it.
Step 2: Now you can edit the trustmark accident claim form. Feel free to use the multifunctional toolbar to add, erase, and transform the content of the form.
The following areas are inside the PDF template you will be filling out.
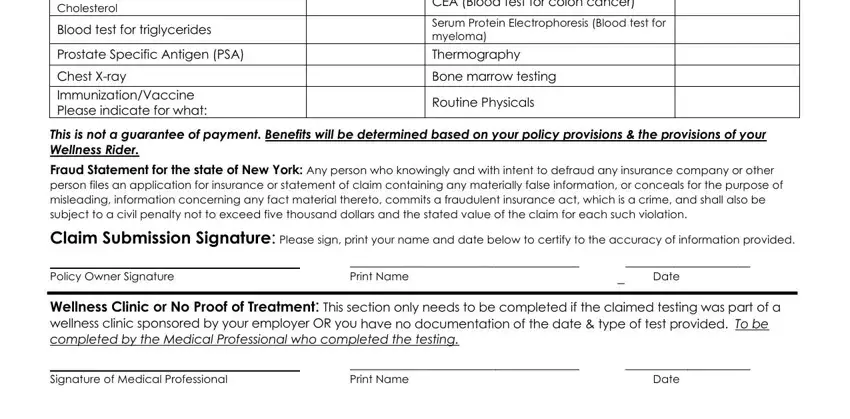
Provide the requested details in the field Fasting blood glucose test Blood, Blood test for triglycerides, Prostate Specific Antigen PSA, Chest Xray ImmunizationVaccine, CEA Blood test for colon cancer, Serum Protein Electrophoresis, Bone marrow testing, Routine Physicals, This is not a guarantee of payment, Fraud Statement for the state of, Claim Submission Signature Please, Policy Owner Signature, Print Name, Date, and Wellness Clinic or No Proof of.
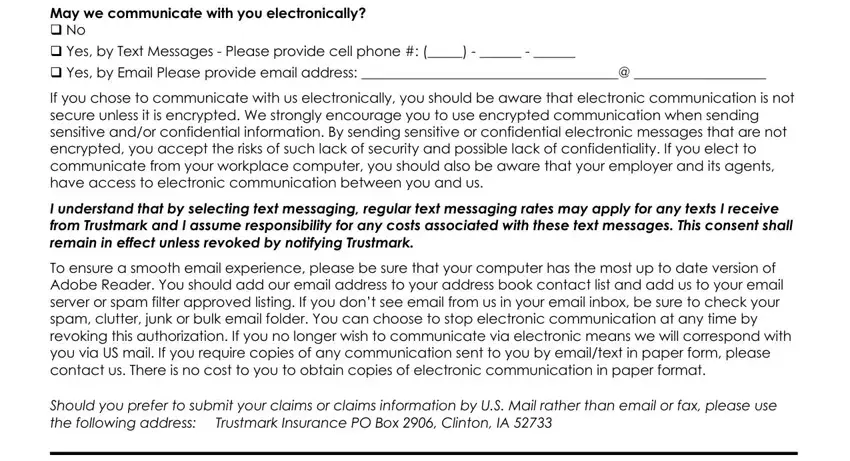
You may be asked to provide the details to let the system complete the segment May we communicate with you, q Yes by Email Please provide, If you chose to communicate with, I understand that by selecting, To ensure a smooth email, and Should you prefer to submit your.
In part Authorization I may revoke or, Policy Owner Signature, Date, Printed Name, Social Security Number, Wellness Rider Claim Form Rider VS, and Page, specify the rights and responsibilities.
Finish by reviewing the following sections and submitting the suitable information: Please complete this authorization, SSN, Claimant Name if appropriate, Policy Numbers, Name Relationship of Third Party, All information all policy and, Only the following information, Name Relationship of Third Party, All information all policy and, Only the following information, My Agent Name of Agent, All information all policy and, My Employer Name of Agent, All information all policy and, and Restrictions may include a.
Step 3: After you have clicked the Done button, your document is going to be obtainable for upload to any electronic device or email you indicate.
Step 4: Get duplicates of the form. It will prevent upcoming worries. We cannot view or publish your details, therefore feel comfortable knowing it will be safe.
