The application process for the Servicemembers' Group Life Insurance Traumatic Injury Protection (TSGLI) is detailed and comprehensive, designed to support members of the military who have suffered severe injuries under traumatic circumstances, with benefits that can provide crucial financial assistance during recovery. The TSGLI program, an essential rider to Service members’ Group Life Insurance (SGLI), recognizes a wide range of traumatic injuries, offering payments between $25,000 and $100,000 depending on the nature and severity of the injuries sustained. To be deemed eligible, service members must have experienced a qualifying traumatic event leading to significant physical harm while insured under SGLI. Notably, eligibility extends retroactively to those injured between October 7, 2001, and November 30, 2005, in the operations areas of Operation Enduring Freedom or Operation Iraqi Freedom. Claimants are guided through a three-step filing procedure requiring documentation from both the service member (or their guardian, power of attorney, or military trustee) and a medical professional to substantiate the claim. The process underscores the importance of accurate and complete submissions to the respective branch of service's TSGLI office, with detailed instructions provided for each section of the claim form to streamline the process. Decisions on claims are made by the branch of service TSGLI office, with payments facilitated directly to the service member or, in specific cases, to an appointed individual acting on their behalf. This structured process ensures that support reaches those in need, underscoring the program's role in mitigating the financial strains that often accompany recovery from severe injuries.
| Question | Answer |
|---|---|
| Form Name | Tsgli Claim Form |
| Form Length | 13 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 3 min 15 sec |
| Other names | 2005, ADL, tsgli application, SERVICEMEMBERS |

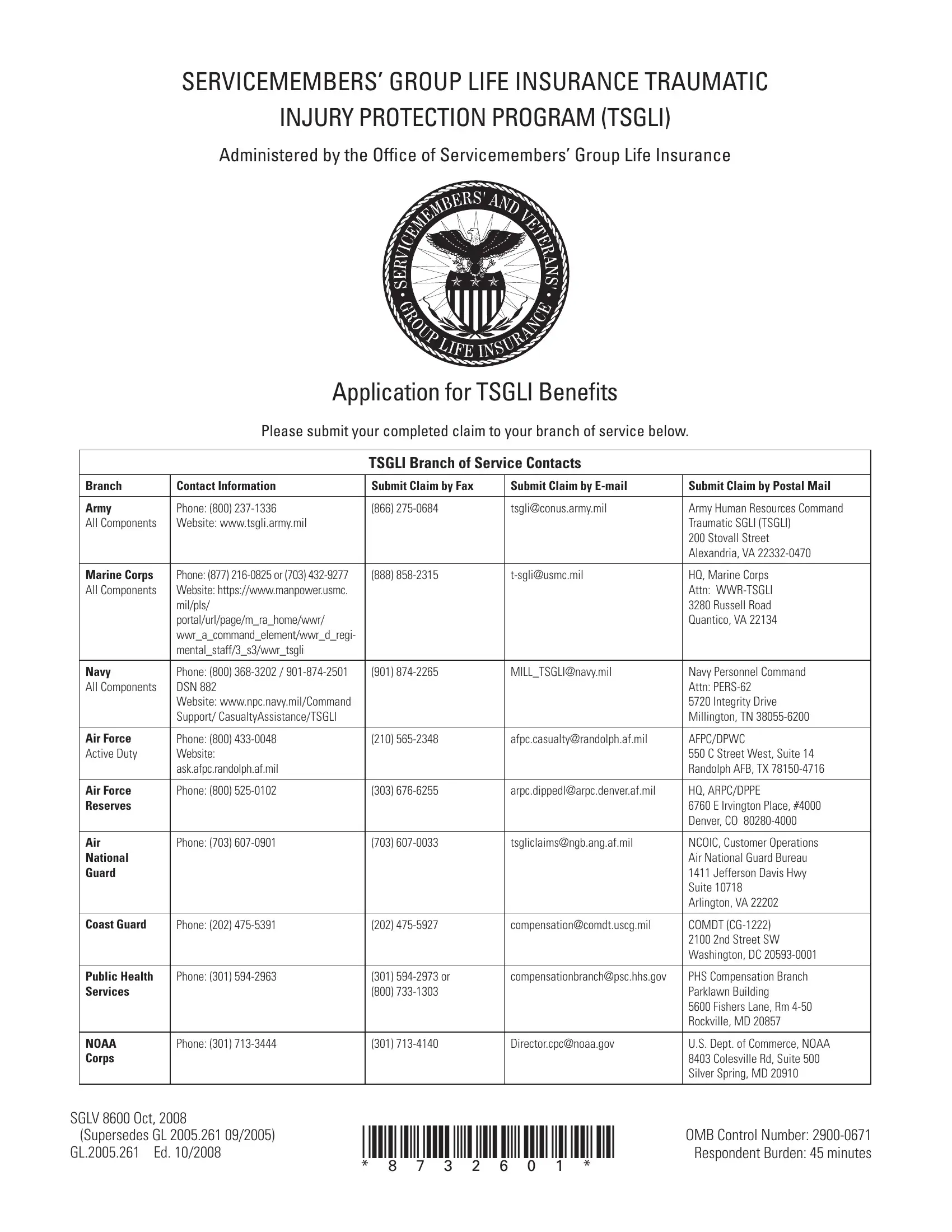
SERVICEMEMBERS’ GROUP LIFE INSURANCE TRAUMATIC
INJURY PROTECTION PROGRAM (TSGLI)
Administered by the Office of Servicemembers’ Group Life Insurance
|
|
Application for TSGLI Benefits |
|
|||||||||||
|
|
Please submit your completed claim to your branch of service below. |
||||||||||||
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
TSGLI Branch of Service Contacts |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|||||
|
Branch |
Contact Information |
|
|
Submit Claim by Fax |
|
|
Submit Claim by |
Submit Claim by Postal Mail |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Army |
Phone: (800) |
|
|
(866) |
|
|
|
|
tsgli@conus.army.mil |
Army Human Resources Command |
|||
|
All Components |
Website: www.tsgli.army.mil |
|
|
|
|
|
|
|
|
|
|
|
Traumatic SGLI (TSGLI) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
200 Stovall Street |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Alexandria, VA |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Marine Corps |
Phone: (877) |
|
|
(888) |
|
|
|
|
HQ, Marine Corps |
||||
|
All Components |
Website: https://www.manpower.usmc. |
|
|
|
|
|
|
|
|
|
|
|
Attn: |
|
|
mil/pls/ |
|
|
|
|
|
|
|
|
|
|
|
3280 Russell Road |
|
|
portal/url/page/m_ra_home/wwr/ |
|
|
|
|
|
|
|
|
|
|
|
Quantico, VA 22134 |
|
|
wwr_a_command_element/wwr_d_regi- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
mental_staff/3_s3/wwr_tsgli |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Navy |
Phone: (800) |
|
|
(901) |
|
|
|
|
MILL_TSGLI@navy.mil |
Navy Personnel Command |
|||
|
All Components |
DSN 882 |
|
|
|
|
|
|
|
|
|
|
|
Attn: |
|
|
Website: www.npc.navy.mil/Command |
|
|
|
|
|
|
|
|
|
|
|
5720 Integrity Drive |
|
|
Support/ CasualtyAssistance/TSGLI |
|
|
|
|
|
|
|
|
|
|
|
Millington, TN |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Air Force |
Phone: (800) |
|
|
(210) |
|
|
|
|
afpc.casualty@randolph.af.mil |
AFPC/DPWC |
|||
|
Active Duty |
Website: |
|
|
|
|
|
|
|
|
|
|
|
550 C Street West, Suite 14 |
|
|
ask.afpc.randolph.af.mil |
|
|
|
|
|
|
|
|
|
|
|
Randolph AFB, TX |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Air Force |
Phone: (800) |
|
|
(303) |
|
|
|
|
arpc.dippedl@arpc.denver.af.mil |
HQ, ARPC/DPPE |
|||
|
Reserves |
|
|
|
|
|
|
|
|
|
|
|
|
6760 E Irvington Place, #4000 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Denver, CO |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Air |
Phone: (703) |
|
|
(703) |
|
|
|
|
tsgliclaims@ngb.ang.af.mil |
NCOIC, Customer Operations |
|||
|
National |
|
|
|
|
|
|
|
|
|
|
|
|
Air National Guard Bureau |
|
Guard |
|
|
|
|
|
|
|
|
|
|
|
|
1411 Jefferson Davis Hwy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Suite 10718 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Arlington, VA 22202 |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Coast Guard |
Phone: (202) |
|
|
(202) |
|
|
|
|
compensation@comdt.uscg.mil |
COMDT |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2100 2nd Street SW |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Washington, DC |
|
|
|
|
|
|
|
|
|
|
|
||||
|
Public Health |
Phone: (301) |
|
|
(301) |
|
|
|
compensationbranch@psc.hhs.gov |
PHS Compensation Branch |
||||
|
Services |
|
|
|
(800) |
|
|
|
|
|
|
|
Parklawn Building |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5600 Fishers Lane, Rm |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Rockville, MD 20857 |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
NOAA |
Phone: (301) |
|
|
(301) |
|
|
|
|
Director.cpc@noaa.gov |
U.S. Dept. of Commerce, NOAA |
|||
|
Corps |
|
|
|
|
|
|
|
|
|
|
|
|
8403 Colesville Rd, Suite 500 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Silver Spring, MD 20910 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SGLV 8600 Oct, 2008 |
*8732601* |
Respondent Burden: 45 minutes |
||||||||||||
GL.2005.261 Ed. 10/2008 |
||||||||||||||
|
(Supersedes GL 2005.261 09/2005) |
|
|
|
|
|
|
|
|
|
|
|
OMB Control Number: |
|
|
|
|
* |
8 |
7 |
3 |
2 |
6 |
0 |
1 |
* |
|
||
GENERAL INFORMATION
The Servicemembers’ Group Life Insurance Traumatic Injury Protection (TSGLI) program is a rider to Service member’s Group Life Insurance (SGLI). The TSGLI rider provides for payment to service members who are severely injured (on or off duty) as the result of a traumatic event and suffer
a loss that qualifies for payment under TSGLI. TSGLI is designed to help traumatically injured service members and their families with financial burdens associated with recovering from a severe injury. TSGLI payments range from $25,000 to $100,000 based on the qualifying loss suffered.
WHO IS ELIGIBLE?
Effective December 1, 2005, all service members who are insured under SGLI and …
n experience a traumatic event
n that results in a traumatic injury
n which is listed as a qualifying loss
are eligible to receive a TSGLI payment. Service members who were severely injured between October 7, 2001, and November 30, 2005, in the theaters of operation for Operation Enduring Freedom or Operation Iraqi Freedom may also be eligible for a TSGLI payment. Members should contact their branch of service for more information.
What is a Traumatic Event?
A traumatic event is the application of external force, violence, chemical, biological, or radiological weapons, accidental ingestion of a contaminated substance, or exposure to the elements that causes damage to your body.
What is a Traumatic Injury?
A traumatic injury is the physical damage to your body that results from a traumatic event.
What is a Qualifying Loss?
A qualifying loss is a traumatic injury that is listed on the TSGLI Schedule of Losses, which lists all covered losses and payment amounts. You may view the complete Schedule of Losses and other TSGLI information at www.insurance.va.gov/sgliSite/TSGLI.htm Your branch of service TSGLI office will determine whether your injury is a qualifying loss for TSGLI purposes.
HOW TO FILE A TSGLI CLAIM
Filing a TSGLI claim is a
Step 1 |
Step 2 |
Step 3 |
|
|
|
The service member [or guardian, power of |
The medical professional… |
The medical professional OR the service member [or |
attorney or military trustee]… |
|
guardian, power of attorney or military trustee]… |
|
|
|
must complete Part A (pages 3 through 6) of the |
must complete Part B (pages 7 through 12). |
must forward Parts A & B to the member’s branch |
form and give it to a medical professional to |
|
of service TSGLI office listed on the front cover of |
complete Part B. Note: If a guardian or power |
|
this form. |
of attorney completes Part A, they must include |
|
|
copies of letters of guardianship, letters of |
|
|
conservatorship, power of attorney, or durable |
|
|
power of attorney (if appropriate). |
|
|
|
|
|
SGLV 8600 Oct, 2008 |
|
*8732602* |
Page 1 |
GL.2005.261 Ed. 10/2008 |
|
||
(Supersedes GL 2005.261 |
09/2005) |
|
|
* 8 7 3 2 6 0 2 *

COMPLETING THE FORM
Instructions on completing the TSGLI Claim Form are included in each section. When completing the form, the service member, guardian, power of attorney or military trustee must complete the service member’s Social Security number on each page of the form. If you have questions about completing the form or if the member is deceased, please contact the branch of service TSGLI office listed on the front cover of this form.
CLAIM DECISION AND PAYMENT
Who Makes the Decision on My Claim?
Your branch of service TSGLI office will make the decision on your claim based upon the information in Parts A and B of the TSGLI Claim Form. They will then forward their decision to the Office of Servicemembers’ Group Life Insurance (OSGLI) for appropriate action.
Who Will Receive the TSGLI Payment?
Payment will be made directly to the member. If the member is incompetent, payment will be made under the appropriate letters of guardianship/ conservatorship or a power of attorney to the guardian, power of attorney or military trustee on the member’s behalf. If the member dies after qualifying for payment, the payment will be made to the member’s current listed SGLI beneficiary(ies). The member must survive for seven days (168 hours) from the date of the traumatic event to be eligible for TSGLI.
How the TSGLI Payment Will be Made?
If your branch of service TSGLI office approves your claim, OSGLI will make the TSGLI benefit payment. There are three payment methods used for TSGLI benefits: Prudential’s Alliance Account®*, Electronic Funds Transfer (EFT), or check.
1.Prudential’s Alliance Account®* — (for member only) An
2.Electronic Funds Transfer (EFT) — Your bank account will be electronically credited with the TSGLI payment amount. Depending on your bank, payments will be credited three to five days from the date the payment is authorized.
Note: If the member does not choose EFT and there is no guardian, power of attorney or military trustee, the payment will be made through Prudential’s Alliance Account.
3.Check Payment — (for guardian, power of attorney or military trustee only) A check will be issued to the guardian or power of attorney or military trustee on behalf of the member.
RESPONDENT BURDEN: We need this information to allow service members who are insured under Servicemembers Group Life Insurance and suffer a loss from a traumatic injury to receive monetary compensation. Title 38, United States Code, allows us to ask for this information. We estimate that you will need an average of 45 minutes to review the instructions, find the information, and complete this form. VA cannot conduct or sponsor a collection of information unless a valid OMB control number is displayed. You are not required to respond to a collection of information if this number is not displayed. Valid OMB control numbers can be located on the OMB Internet Page at www.whitehouse.gov/omb/library/ OMBINV.html#VA. If desired, you can call
PRIVACY ACT NOTICE: VA will not disclose information collected on this survey to any source other than what has been authorized under the Privacy Act of 1974 or Title 38, Code of Federal Regulations 1.576 for routine uses identified in the VA system of records , 36VA00, Veterans and Armed Forces Personnel U.S. Government Life Insurance
1980A. VA will not deny an individual benefits for refusing to provide his or her Social Security number unless the disclosure is required by a Federal Statute of law in effect prior to January 1, 1975, and still in effect.
*Open Solutions BIS, Inc. is the Administrator of the Prudential Alliance Account Settlement Option, a contractual obligation of The Prudential Insurance Company of America, located at 751 Broad Street, Newark, NJ
SGLV 8600 Oct, 2008 |
|
*8732603* |
Page 2 |
GL.2005.261 Ed. 10/2008 |
|
||
(Supersedes GL 2005.261 |
09/2005) |
|
|
* 8 7 3 2 6 0 3 *