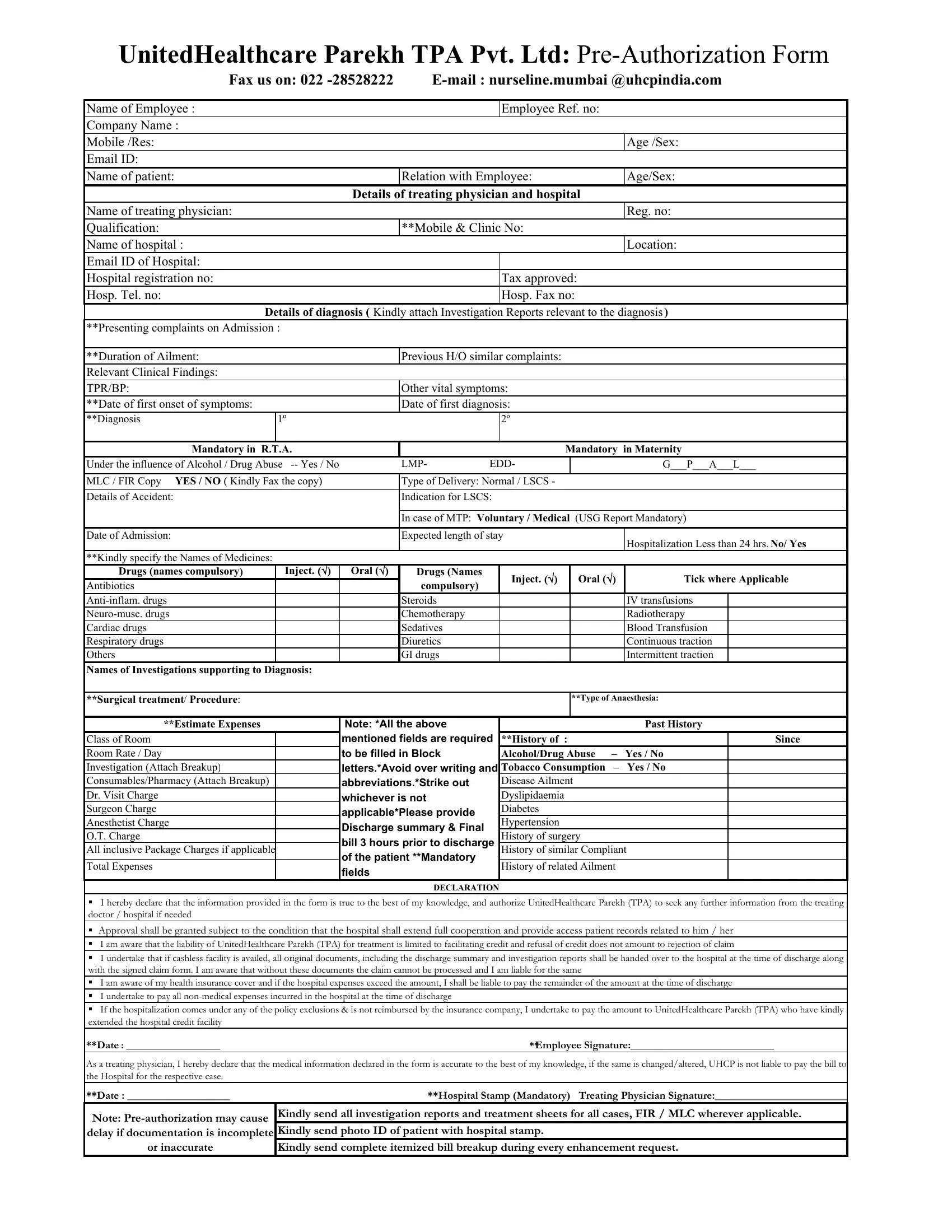
At the heart of healthcare management, especially when dealing with insurance claims and pre-authorizations, lies a complex network of procedural necessities aimed at ensuring both accuracy and compliance with policy stipulations. The United Healthcare Parekh Claim form serves as a critical instrument within this network, facilitating the seamless processing of insurance claims for employees needing medical services. This form encompasses a comprehensive range of details starting from basic identifiers such as the name of the employee, employee reference number, and company name, to more nuanced information including the patient's relation to the employee, details of the treating physician, and the hospital's credentials. It meticulously captures every aspect of the medical condition or incident leading to the claim, including diagnosis, treatment details, expected stay duration, and a declaration section for both the claimant and the treating physician, affirming the authenticity of the information provided. The form mandates the submission of investigation reports supporting the diagnosis, a detailed account of drugs and procedures employed, and a breakdown of the estimated expenses, covering the room charges and all inclusive package charges if applicable. Moreover, it underscores the conditions under which approval for claims might be granted or denied, highlighting the necessity for full cooperation from the hospital in providing access to patient records. By filling out this form, employees initiate the process toward availing themselves of the healthcare benefits as stipulated in their insurance coverage, hence underscoring the importance of accuracy and thoroughness in its completion.
| Question | Answer |
|---|---|
| Form Name | United Healthcare Parekh Claim Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | united health parekh claim form, unitedhealthcare preauth form, united healthcare parekh preauth form download, united health care parekh claim form |
