The procedure of filling in the champva 10 10d is fairly easy. We made certain our software is not hard to navigate and can help fill out almost any document within minutes. The following are a couple of steps you need to take:
Step 1: Choose the "Get Form Here" button.
Step 2: It's now possible to modify your champva 10 10d. This multifunctional toolbar permits you to add, eliminate, change, and highlight content material or undertake other sorts of commands.
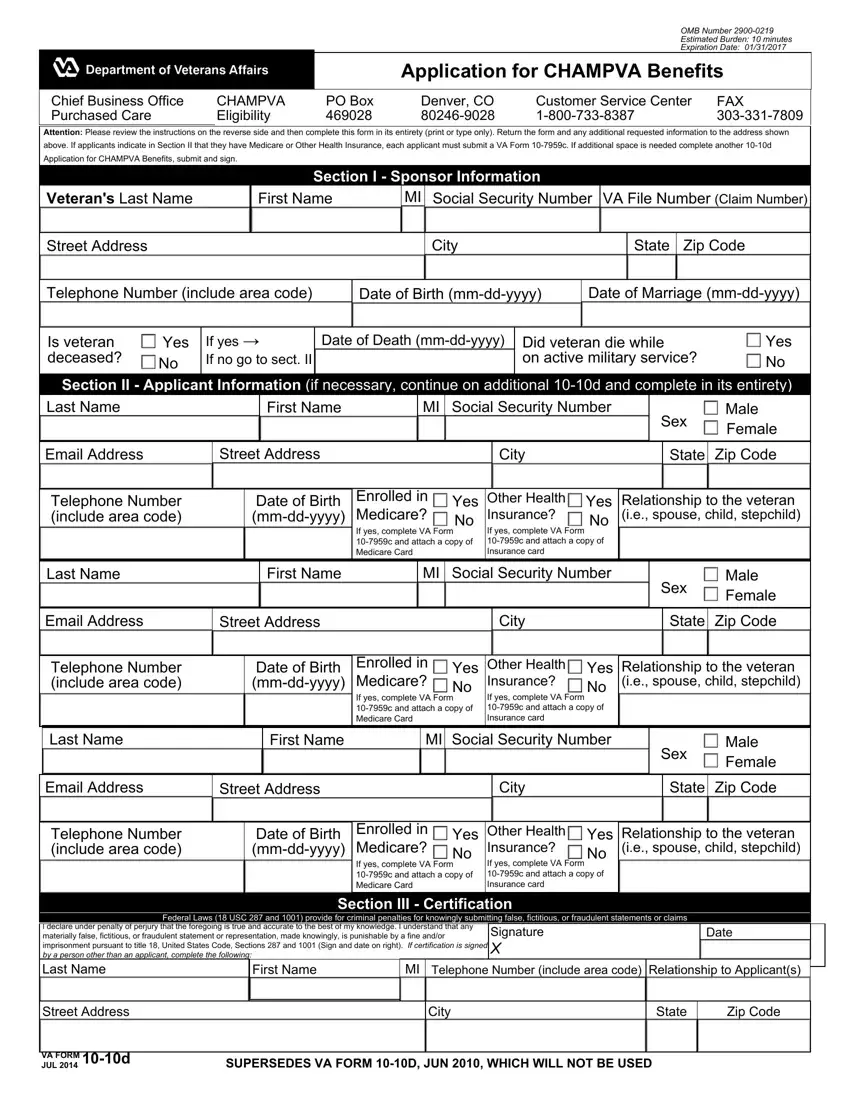
These particular sections are inside the PDF file you will be completing.
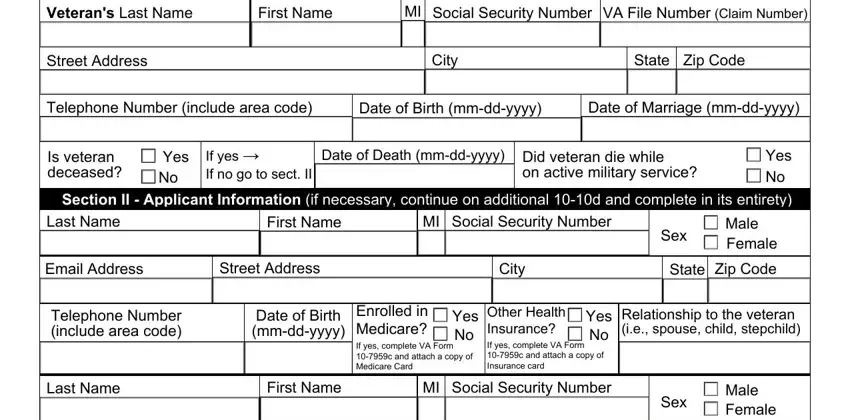
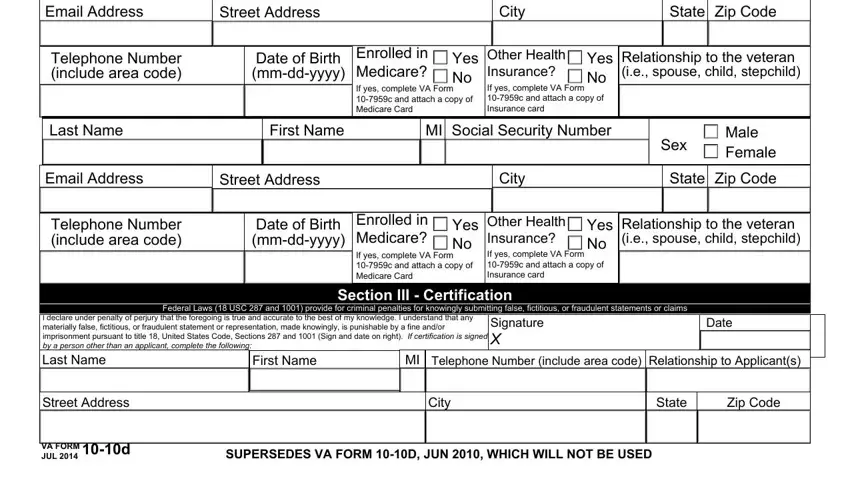
Put down the data in the Email Address, Street Address, City, State Zip Code, Telephone Number include area code, Date of Birth mmddyyyy, Enrolled in Medicare If yes, Yes Other Health No, Yes Relationship to the veteran ie, Last Name, First Name, MI Social Security Number, Email Address, Street Address, and City area.
Write down any particulars you may need within the area Privacy Act Information The, The Paperwork Reduction Act This, Application for CHAMPVA Benefits, and CHAMPVA Eligibility Criteria.
Describe the rights and responsibilities of the sides within the part Spouse Refers to a person who is, Child Includes legitimate adopted, NOTE Except for stepchildren the, School Certification, and In order to extend CHAMPVA.
Step 3: Choose the Done button to save your file. So now it is accessible for upload to your device.
Step 4: Get a minimum of several copies of the document to avoid any specific possible future problems.
