We've used the endeavours of the best computer programmers to make the PDF editor you are about to work with. Our software will allow you to prepare the Va Form 10 10Cg form without any difficulty and don’t waste your time. All you have to do is stick to the next quick tips.
Step 1: To get started, hit the orange button "Get Form Now".
Step 2: When you've accessed the Va Form 10 10Cg editing page you can discover every one of the actions you can use concerning your template from the top menu.
In order to complete the file, type in the details the software will request you to for each of the appropriate sections:
The software will need you to fill in the Veterans who do not meet the, VA FORM APR, and Page of segment.

It is crucial to record some data inside the field Submitting your application Read, Supporting documentation, provided VA Form EZ Application, Submit application to, Program of Comprehensive, THE PAPERWORK REDUCTION ACT, This information collection is in, PRIVACY ACT INFORMATION, and VA is asking you to provide the.
The space Attention Complete the application, Last Name, First Name, Middle Name, SECTION I VETERAN, Social Security NumberTax, Date of Birth MMDDYYYY, Sex, Male, Female, Current Street Address, City, State, Zip Code, and Primary Telephone Number Including should be where you indicate all parties' rights and responsibilities.
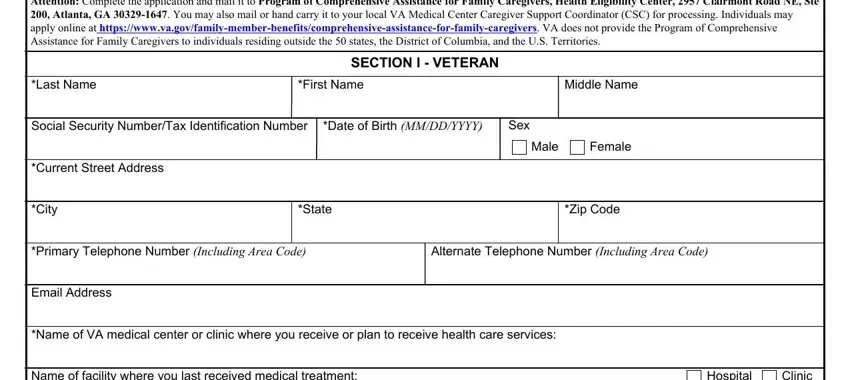
Finalize by checking the next fields and filling them out as needed: Name of facility where you last, Hospital, Clinic, Federal Laws USC and provide, I certify that I give consent to, Veteran or Representative Signature, Date MMDDYYYY, Last Name, First Name, Middle Name, SECTION II PRIMARY FAMILY, Social Security NumberTax, Date of Birth MMDDYYYY, Sex, and Male.
Step 3: Click "Done". You can now export your PDF form.
Step 4: Just be sure to create as many duplicates of your file as you can to stay away from potential problems.
