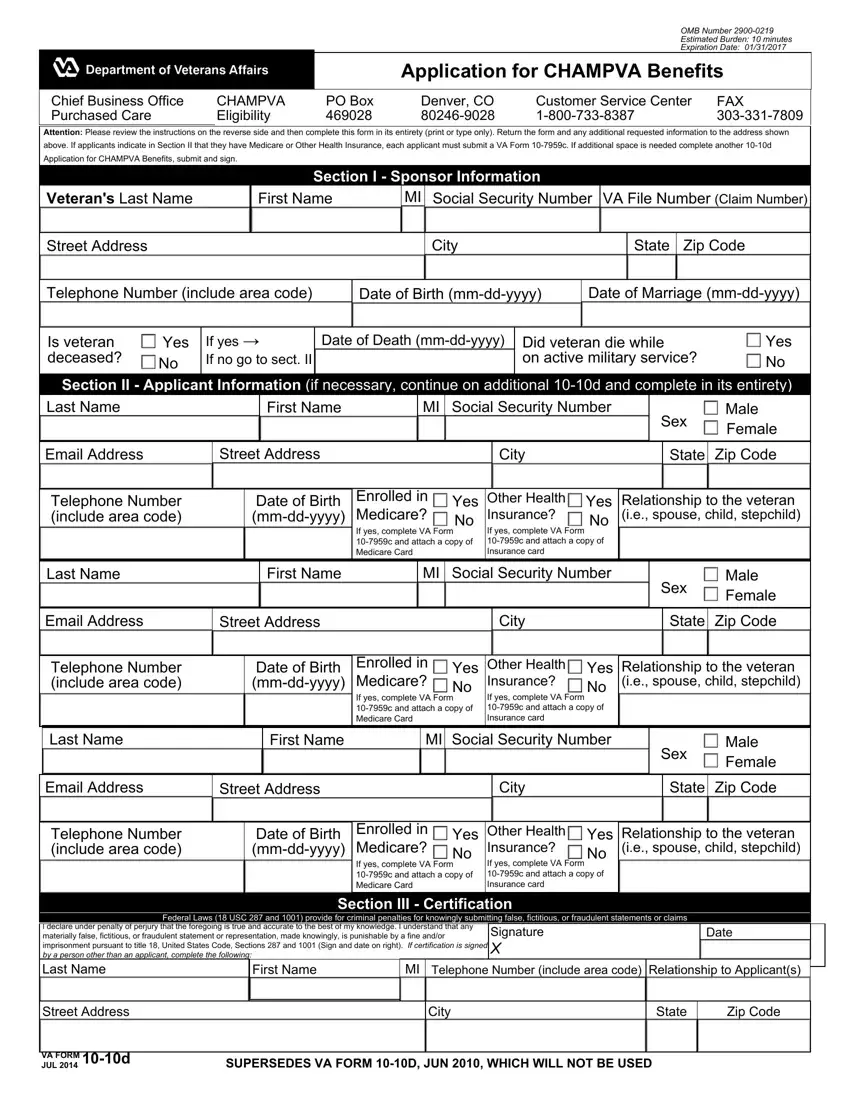
Understanding the complexities and necessities of applying for health benefits can be an arduous task for veterans and their families. The VA CHAMPVA Application 10-10D form is a crucial step for those seeking to obtain CHAMPVA benefits, designed to support the healthcare needs of eligible dependents of veterans. This comprehensive form serves as the initial point of contact between the applicant and the Chief Business Office CHAMPVA, meticulously outlining the information required for processing benefits eligibility. Applicants are instructed to provide detailed information, including the veteran's service and personal data, as well as any relevant Medicare or other health insurance details through specific sections and accompanying forms if necessary. Emphasized within the instructions is the importance of accurately completing the form to ensure timely and correct eligibility determination. The form also outlines the consequences of failing to provide accurate information, highlighting federal laws that deter and penalize fraudulent claims. Furthermore, it briefly touches on eligibility criteria, the impact of Medicare, and defines terms such as ‘service-connected condition/disability’ and 'sponsor,' which are vital for understanding CHAMPVA’s scope. Additionally, it provides instructions for those with changes in their educational or marital status, ensuring they remain compliant with the eligibility requirements. This form not only facilitates access to essential healthcare services for those who have dedicated themselves and their families to the nation's service but also underscores the importance of integrity in applying for such benefits.
| Question | Answer |
|---|---|
| Form Name | Va Champva Application Form 10 10D |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | veterans affairs form champva online, how to veterans affairs champva, champ va, champva 10 10d |
