
 NO
NO

 NO
NO
 NO
NO
 NO
NO
 NO
NO

 YES
YES 
 NO
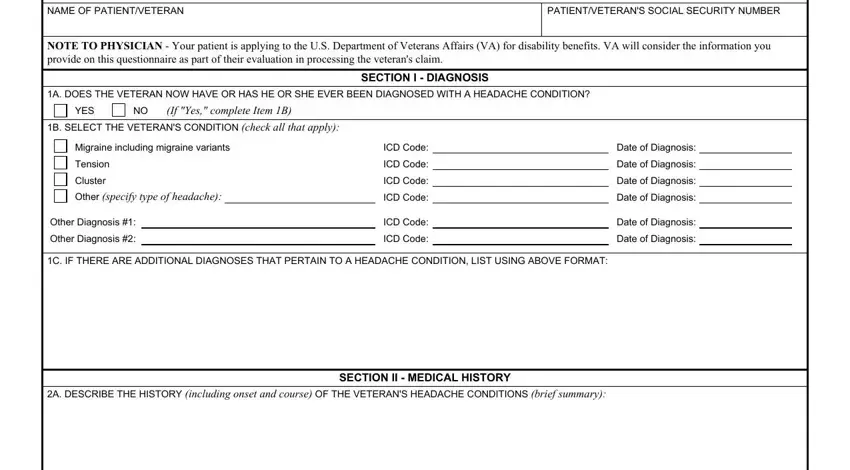
NOThis PDF editor allows you to prepare the migraine dbq form form. You will be able to obtain the file as soon as possible through using these simple actions.
Step 1: You should press the orange "Get Form Now" button at the top of the web page.
Step 2: You can now enhance your migraine dbq form. Feel free to use our multifunctional toolbar to add, delete, and adjust the content of the file.
The next parts will compose the PDF file that you'll be creating:
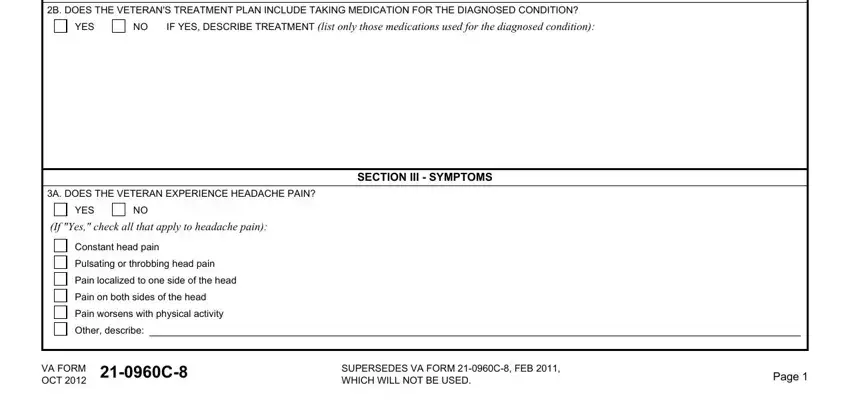
The program will need you to fill out the B DOES THE VETERANS TREATMENT PLAN, YES, IF YES DESCRIBE TREATMENT list, SECTION III SYMPTOMS, A DOES THE VETERAN EXPERIENCE, YES, If Yes check all that apply to, Constant head pain, Pulsating or throbbing head pain, Pain localized to one side of the, Pain on both sides of the head, Pain worsens with physical activity, Other describe, VA FORM OCT C, and SUPERSEDES VA FORM C FEB WHICH box.
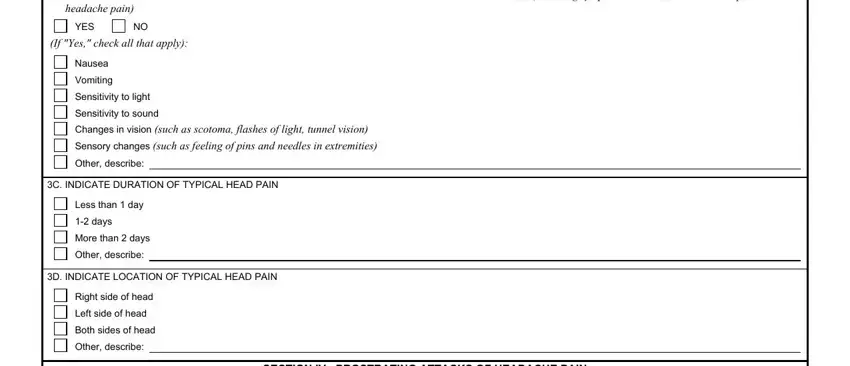
You could be requested for some valuable particulars in order to fill out the B DOES THE VETERAN EXPERIENCE, headache pain, YES, If Yes check all that apply, Nausea, Vomiting, Sensitivity to light, Sensitivity to sound Changes in, Other describe, C INDICATE DURATION OF TYPICAL, Less than day, days, More than days, Other describe, and D INDICATE LOCATION OF TYPICAL section.
The space A MIGRANE DOES THE VETERAN HAVE, SECTION IV PROSTRATING ATTACKS OF, YES, If Yes indicate frequency on, Less than once every months, Once in months, Once every month, More frequently than once per month, B DOES THE VETERAN HAVE VERY, YES, C NONMIGRAINE DOES THE VETERAN, YES, If Yes indicate frequency on, Less than once every months, and Once in months should be where you can include each side's rights and responsibilities.
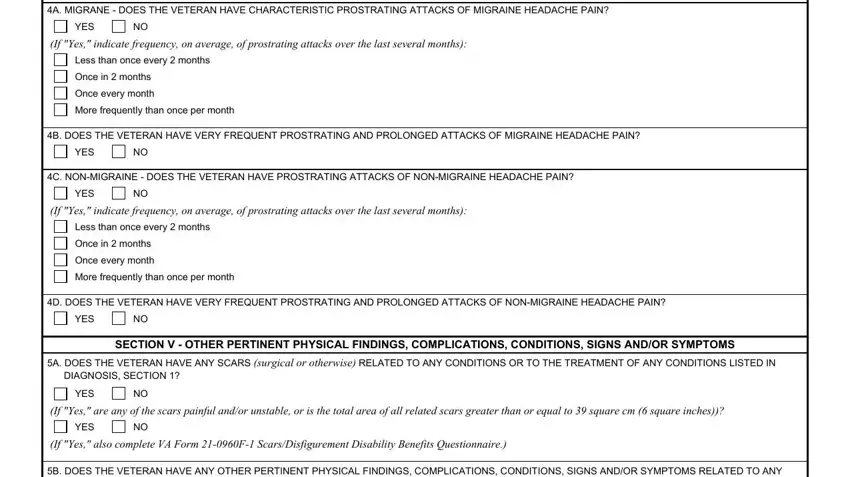
Finish by looking at the following areas and writing the proper particulars: B DOES THE VETERAN HAVE ANY OTHER, CONDITIONS LISTED IN SECTION, YES, If Yes describe in a brief summary, VA FORM C OCT, and Page.

Step 3: As soon as you are done, click the "Done" button to upload the PDF form.
Step 4: Make sure to remain away from possible future problems by making a minimum of two duplicates of your file.
