Filling in virginia initial application licensing is not hard. Our team designed our PDF tool to make it simple to use and help you complete any form online. Here are a couple steps that you should stick to:
Step 1: Discover the button "Get Form Here" and then click it.
Step 2: At the moment you're on the document editing page. You may edit and add information to the form, highlight specified content, cross or check particular words, add images, sign it, get rid of unwanted areas, or take them out altogether.
For every single segment, complete the information asked by the platform.
Fill out the Chief Executive Officer or, NameTitle, Phone Fax Number Email, All Residential Services The, Community Liaison Name Phone, ORGANIZATIONAL STRUCTURE Identify, Check one of the following, ForProfit, Check one of the following, Unincorporated Organization or, State, Community Services Board Other, Public agency, Identify accrediting or certifying, and Accreditation Council for area with the details demanded by the platform.
The program will ask you to present specific significant details to instantly complete the segment APPLICANT PARENT COMPANY, Mailing Address City County State, Zip Phone Email, and NameTitle.
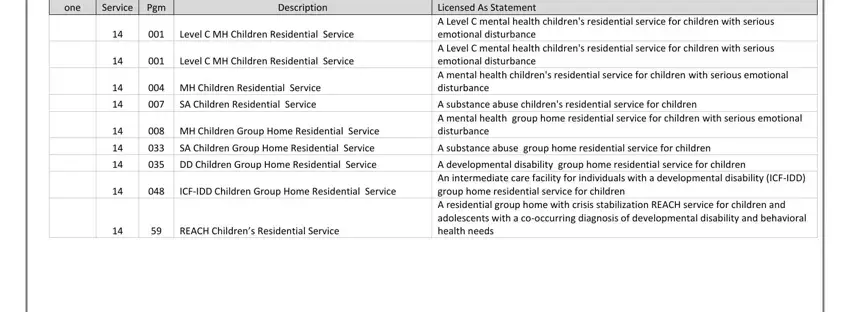
In the field SA Children Group Home Residential, A substance abuse group home, Licensed As Statement A Level C, A substance abuse childrens, A developmental disability group, Check one, Service, Pgm, Description, Level C MH Children Residential, Level C MH Children Residential, MH Children Residential Service, SA Children Residential Service, MH Children Group Home, and DD Children Group Home, describe the rights and obligations of the parties.
Finish by taking a look at the following sections and filling them out as required: SERVICE INFORMATION Complete for, and Developmental Services, Service Director, Phone E Mail, Client Demographics check all that, Male, Female Both Child, Adolescent Min Max Age Range, Location Name of beds, LOCATION, Address, City County State Zip, Location Manager Phone E mail, Directions, and NAME AND ADDRESS OF OWNER OF.
Step 3: Hit the "Done" button. Next, you can export the PDF file - save it to your device or forward it by using electronic mail.
Step 4: Generate duplicates of the document. This may save you from forthcoming worries. We cannot watch or publish your details, as a consequence you can be confident it is secure.
