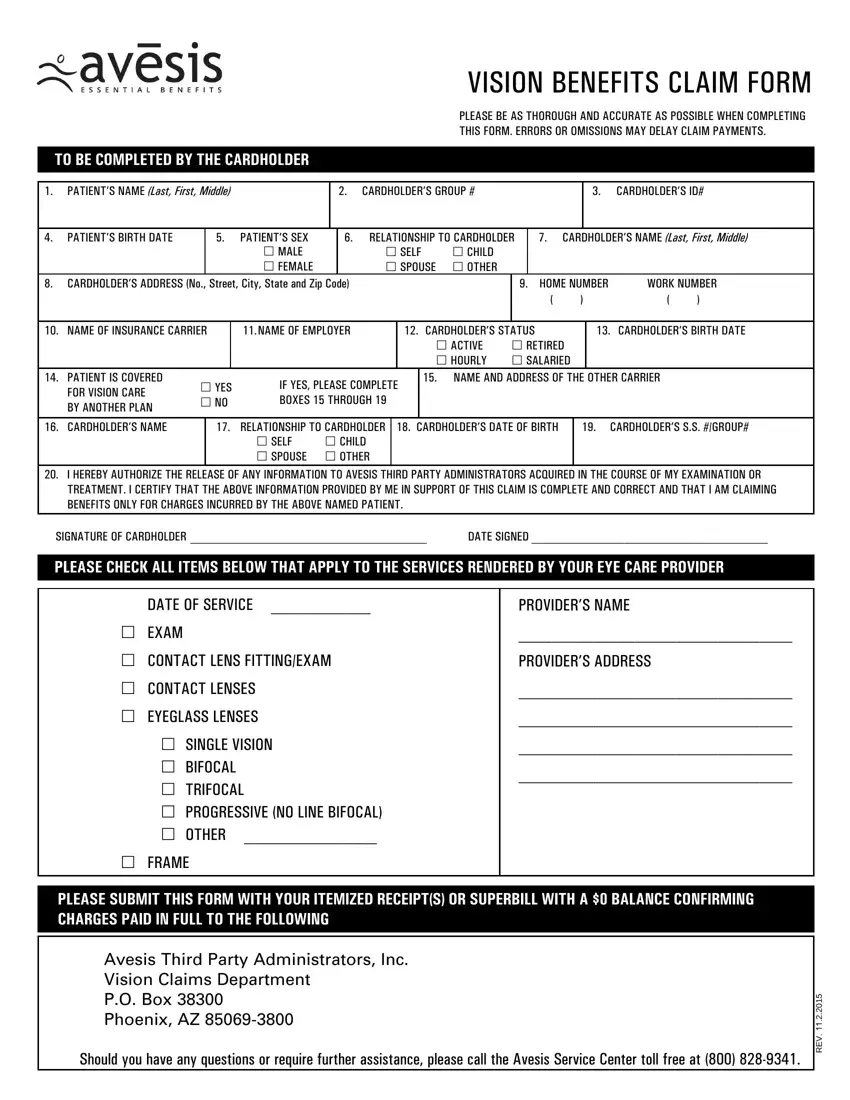
Navigating the terrain of insurance claims can often feel like deciphering an ancient script. Among such forms, the Vision Benefits Claim Form emerges as a critical document for those aiming to secure reimbursements for vision care expenses. This form mandates a meticulous level of accuracy and thoroughness from the cardholder, highlighting the importance of providing correct and complete information to ensure the smooth processing of claims. Essential fields include patient and cardholder details, such as names, identification numbers, and relationships, alongside specifics about the insurance carrier and employer, delineating the pathway to ascertain coverage eligibility. Furthermore, the form opens a window into the detailed universe of vision care, demanding information about the services rendered—ranging from exams to eyewear. Also crucial is the authorization for information release, underpinning the claim's legitimacy, and a declaration ensuring that the information provided is truthful and claims are made solely for incurred charges. Augmenting the form are stark fraud warnings across various states, underscoring the legal implications of submitting fraudulent claims, thereby weaving a tapestry of accountability and precision. Thus, this form not only facilitates the reimbursement process but also diligently guards against insurance fraud, illuminating its multifaceted role in the landscape of vision care insurance.
| Question | Answer |
|---|---|
| Form Name | Vision Benefits Claim Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | claimant, avesis forms, avesis android app, Arizona |
