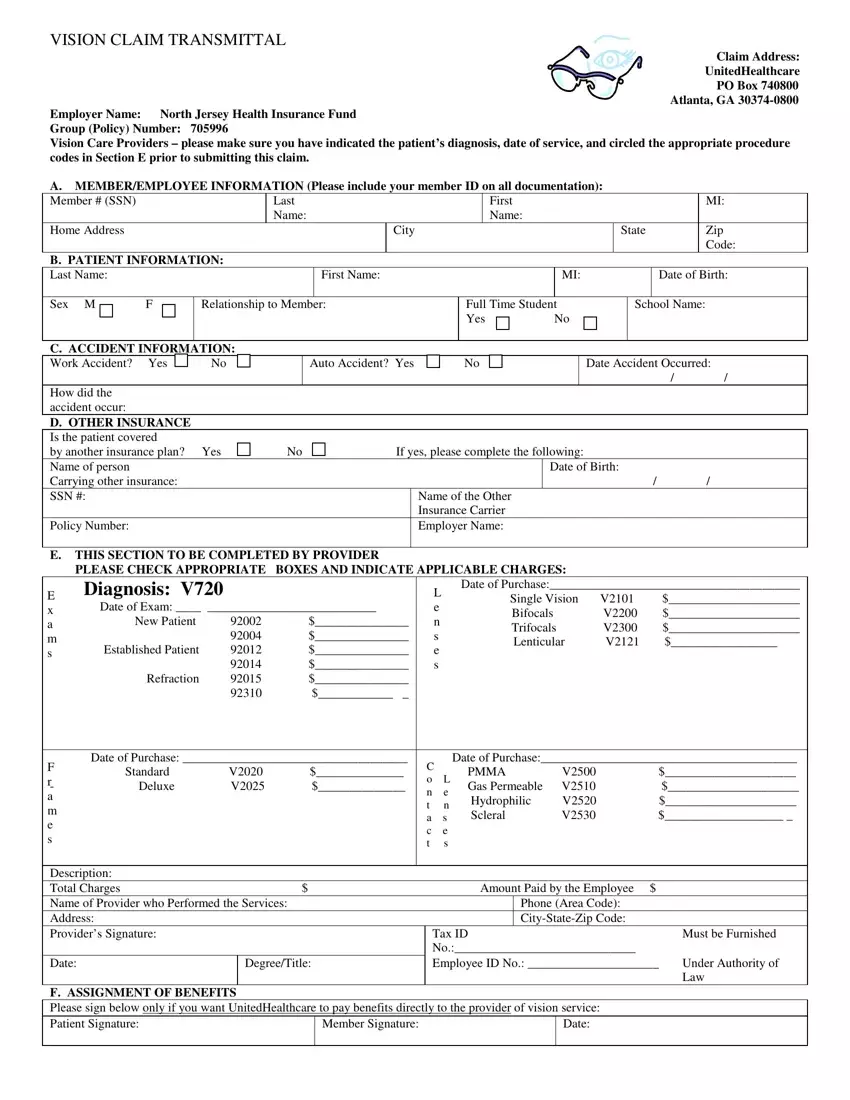
When it comes to vision care claims, ensuring accuracy and completeness in documentation is crucial for a smooth processing experience. The Vision Claim Transmittal form, utilized for submissions to UnitedHealthcare, embodies this principle by guiding both providers and policyholders through a detailed outline of necessary information. Situated at the core of the form are sections dedicated to comprehensive member and patient details, including identification, contact, and insurance information, all designed to streamline the identification and processing of the claim. Noteworthy is the section aimed specifically at vision care providers, mandating the inclusion of a correct patient diagnosis, the date of service, and the precise circling of applicable procedure codes, emphasizing the necessity of precision in health claims submissions. Furthermore, the form addresses scenarios involving accidents, inquiring about their nature and details, an aspect critical for claims tied to specific incidents. It also navigates through the intricacies of dealing with other insurance carriers that may cover the patient, requesting detailed information to ascertain coordination of benefits. Insightfully, the form provides a designated area for providers to list services rendered alongside their associated charges, which plays a pivotal role in determining the claim amount. Significantly, it features an option for the assignment of benefits, which, when opted into, allows for direct payment to service providers, simplifying the reimbursement process. By meticulously filling out this form and ensuring no supplementary documents such as receipts or bills are attached upon submission, claimants enhance the efficiency of the adjudication process, thereby fostering a smoother path to claim resolution.
| Question | Answer |
|---|---|
| Form Name | Vision Claim Transmittal Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | uhc vision claim form, united healthcare reimbursement form vision, united healthcare vision out of network claim form, united healthcare vision reimbursement form |
