You can complete the Cigna Vision Claim Form using our free online PDF editor. Follow the steps below to fill out and save your form.
Step 1: Open the form. Click the "Get Form Here" button at the top of this page. The form will open in the FormsPal PDF editor.
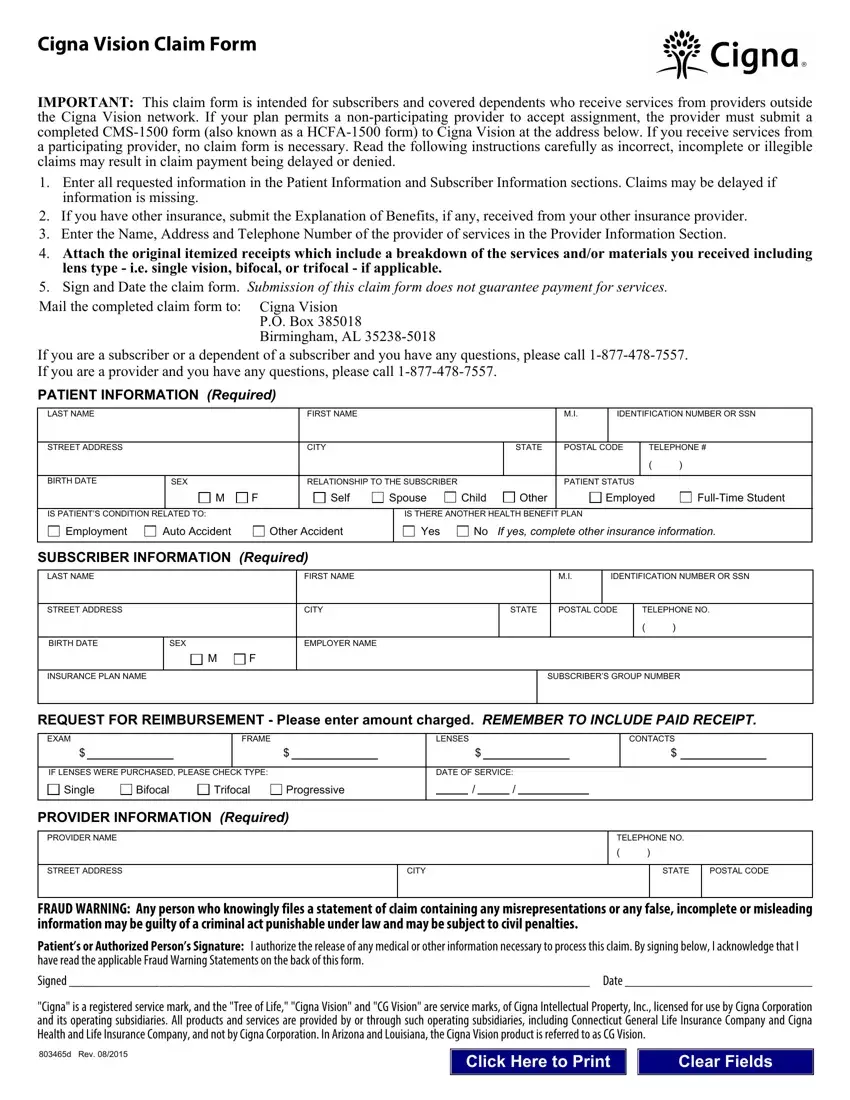
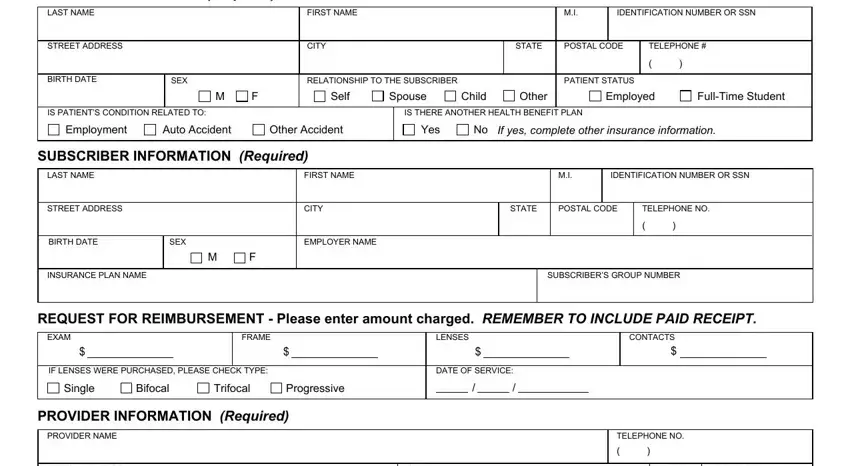
Step 2: Fill in your information. Enter your name, address, and Cigna subscriber ID number. Add the date of service and your provider's contact information. Use the editing tools to type in fields, check boxes, add a signature, and highlight key sections.
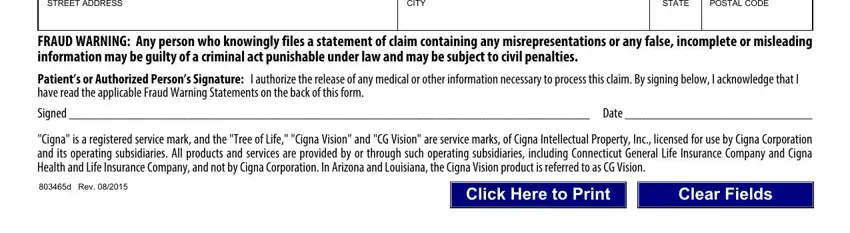
Fill in the STREET ADDRESS, CITY, STATE, and POSTAL CODE fields for your provider. Read the FRAUD WARNING section carefully. Sign in the Patients or Authorized Persons area. The form includes the note that Cigna is a registered service mark.
Step 3: Review and finalize. Check that all fields are filled in clearly and completely. Attach copies of your itemized receipts and your provider's statement. If you have other insurance, include an Explanation of Benefits.
Step 4: Download and submit. Click the Done button to save your completed form. Download it as a PDF, print it, or send it by email. Mail the completed form to the address on the last page of the form.
You can save a copy for your records. FormsPal does not store or share your personal information.
Need help with other Cigna forms? See the Cigna Gym Reimbursement Form or the Cigna Dental Enrollment Form.
