

Any time you would like to fill out selecting, there's no need to download and install any kind of applications - just give a try to our online PDF editor. Our editor is constantly developing to provide the best user experience attainable, and that's thanks to our commitment to constant enhancement and listening closely to customer opinions. Should you be looking to get started, here is what it requires:
Step 1: Just click the "Get Form Button" at the top of this site to see our pdf file editor. This way, you will find everything that is needed to fill out your file.
Step 2: This editor will allow you to work with your PDF file in a variety of ways. Change it with your own text, correct what's already in the document, and put in a signature - all at your disposal!
It really is simple to complete the pdf with our practical guide! Here is what you need to do:
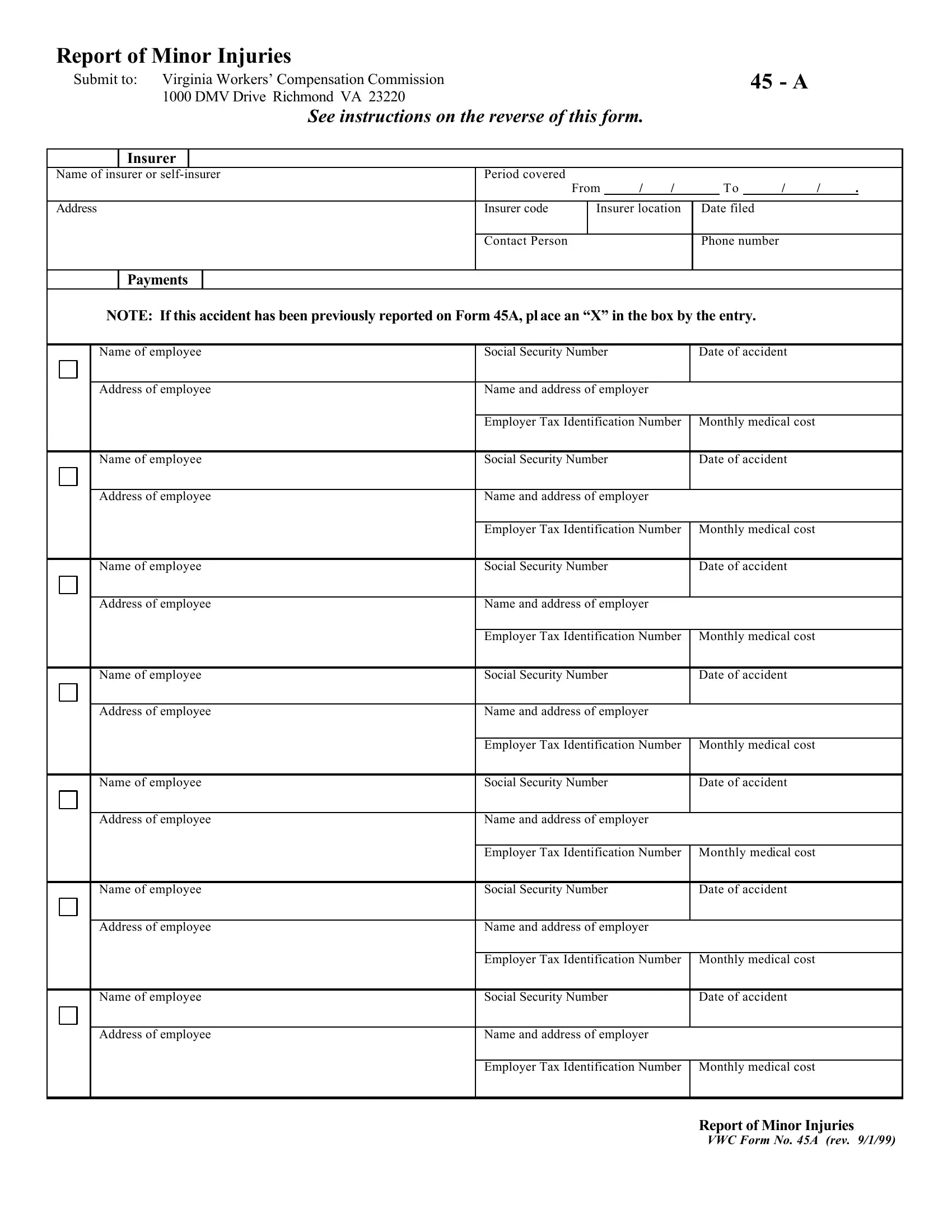
1. Before anything else, when filling in the selecting, begin with the area that includes the subsequent fields:
2. Just after filling in the previous section, head on to the next part and enter the necessary particulars in all these blank fields - Address of employee Name of, Address of employee Name of, Address of employee Name of, Social Security Number Name and, Social Security Number Name and, Date of accident, Social Security Number, Date of accident, Name and address of employer, Social Security Number, Date of accident, Name and address of employer, Social Security Number Name and, and Date of accident.
Always be really mindful when filling out Social Security Number Name and and Name and address of employer, because this is the section where a lot of people make a few mistakes.
3. This stage is going to be straightforward - complete every one of the blanks in Address of employee Name of, Social Security Number Name and, Date of accident, Report of Minor Injuries, and VWC Form No A rev in order to complete this segment.
Step 3: Spell-check the details you've inserted in the blank fields and then hit the "Done" button. Grab your selecting as soon as you subscribe to a 7-day free trial. Conveniently view the pdf inside your personal account, along with any edits and changes conveniently preserved! We don't share or sell the details that you use while dealing with documents at our website.