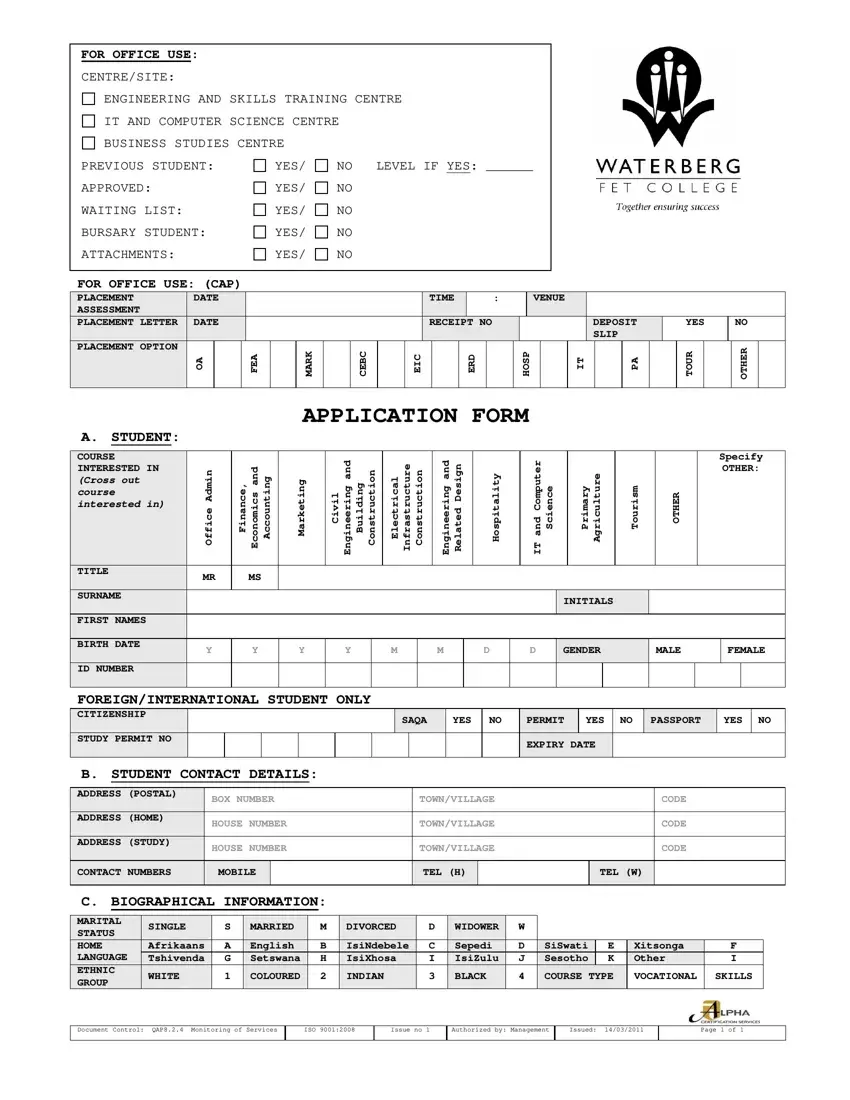
Enrolling at Waterberg Fet College is a significant step towards achieving one's educational and career goals, requiring careful completion of their application form. This comprehensive document serves multiple purposes, guiding both prospective students and the college administration through the application process. It covers a broad range of information, starting from basic personal details such as name, birth date, and contact information, to more specific educational and health-related data. The form is thoughtfully designed to assess the suitability of candidates for various courses ranging from engineering and skills training to business studies, IT, and more, ensuring each student finds their best fit. Notably, it includes sections for office use only, highlighting areas such as placement status, bursary eligibility, and required attachments, which are crucial for internal tracking and decision-making. Understanding personal backgrounds, including biographical and medical information, further allows the college to accommodate diverse needs, ensuring a supportive learning environment. Additionally, it requests details of a parent, guardian, or next of kin, ensuring a reliable point of contact. The form even addresses the need for hostel accommodation, making it clear that the college aims to facilitate a comprehensive support system for students. All applicants are reminded to provide essential documents, such as their highest grade results and identification paperwork, emphasizing the college’s commitment to thorough and inclusive education access. With a clear understanding of the form’s sections and the importance of each, applicants are well-equipped to embark on this exciting educational journey.
| Question | Answer |
|---|---|
| Form Name | Waterberg Fet College Application Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | waterberg tvet college online application 2021 lebowakgomo, mokopane tvet college online application, thabazimbi tvet college online application, mokopane tvet college online application 2021 |
