
Dealing with PDF forms online is actually super easy with our PDF tool. Anyone can fill in michigan workers compensation application here painlessly. Our editor is consistently developing to provide the very best user experience achievable, and that's because of our dedication to constant enhancement and listening closely to feedback from customers. In case you are looking to get going, here is what it will take:
Step 1: Just click the "Get Form Button" above on this webpage to access our pdf editing tool. There you'll find all that is needed to work with your document.
Step 2: This editor provides you with the capability to modify PDF files in a range of ways. Change it with customized text, correct original content, and place in a signature - all manageable in minutes!
When it comes to fields of this specific document, this is what you need to do:
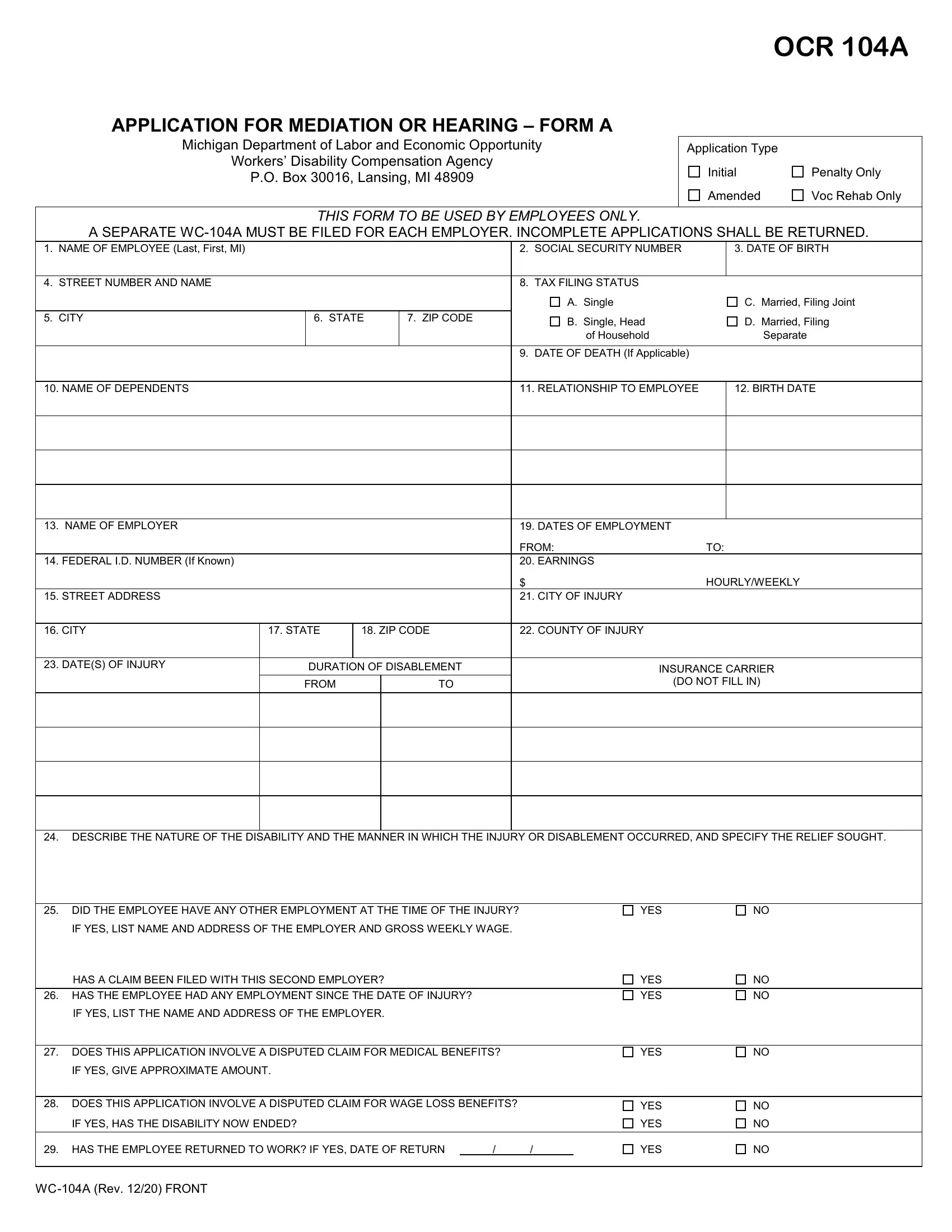
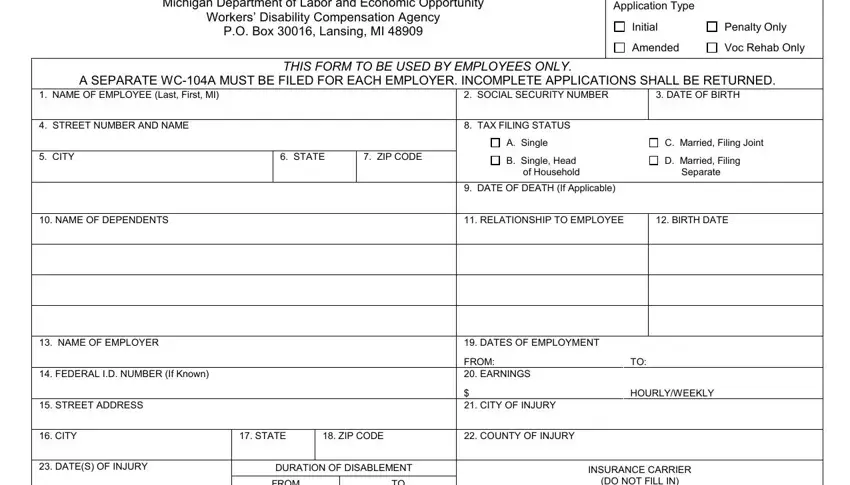
1. The michigan workers compensation application necessitates specific information to be typed in. Be sure the following blanks are filled out:
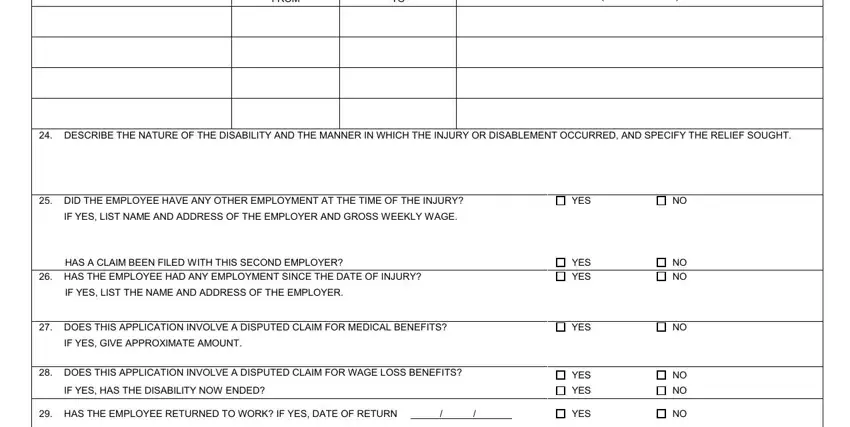
2. When the last array of fields is complete, you're ready add the needed specifics in FROM, DO NOT FILL IN, DESCRIBE THE NATURE OF THE, DID THE EMPLOYEE HAVE ANY OTHER, IF YES LIST NAME AND ADDRESS OF, YES, HAS A CLAIM BEEN FILED WITH THIS, HAS THE EMPLOYEE HAD ANY, YES YES, NO NO, IF YES LIST THE NAME AND ADDRESS, DOES THIS APPLICATION INVOLVE A, IF YES GIVE APPROXIMATE AMOUNT, DOES THIS APPLICATION INVOLVE A, and IF YES HAS THE DISABILITY NOW ENDED in order to move forward further.
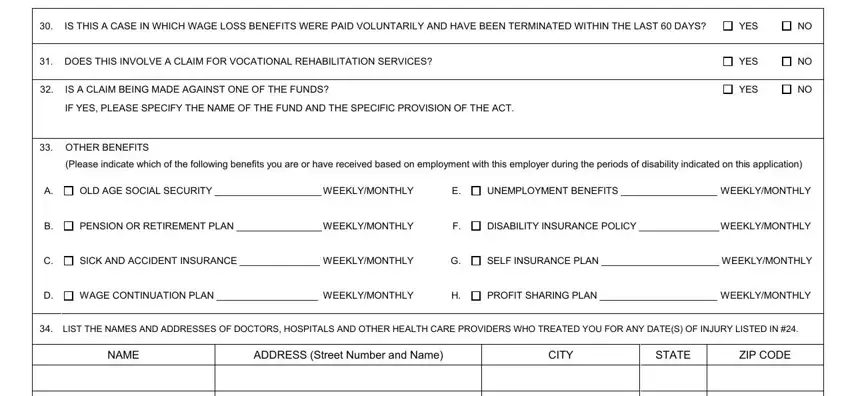
3. This next step should also be quite uncomplicated, IS THIS A CASE IN WHICH WAGE LOSS, YES, DOES THIS INVOLVE A CLAIM FOR, IS A CLAIM BEING MADE AGAINST ONE, IF YES PLEASE SPECIFY THE NAME OF, YES, YES, OTHER BENEFITS, Please indicate which of the, OLD AGE SOCIAL SECURITY, PENSION OR RETIREMENT PLAN, SICK AND ACCIDENT INSURANCE, WAGE CONTINUATION PLAN, UNEMPLOYMENT BENEFITS, and DISABILITY INSURANCE POLICY - every one of these empty fields has to be filled out here.
4. Completing LIST THE NAMES AND ADDRESSES OF, NAME, ADDRESS Street Number and Name, CITY, STATE, ZIP CODE, I INTEND TO CALL WITNESSES WHO, Yes, Making a false or fraudulent, Workers Disability Compensation, AUTHORITY COMPLETION PENALTY, SIGNATURE OF APPLICANT, TELEPHONE NUMBER, and DATE is vital in this fourth form section - ensure to don't rush and be mindful with every blank area!
A lot of people frequently make mistakes while filling in TELEPHONE NUMBER in this section. You should definitely review everything you enter here.
5. This form needs to be wrapped up by going through this area. Here you'll find a full set of form fields that require specific information to allow your document submission to be accomplished: ATTORNEY IDENTIFICATION NAME OF, ADDRESS Street Number and Name, NAME OF LAW FIRM, ATTORNEY ID, CITY, STATE, ZIP CODE, SIGNATURE OF ATTORNEY, TELEPHONE NUMBER, DATE, and WCA Rev BACK.
Step 3: Just after double-checking your entries, hit "Done" and you're all set! Make a 7-day free trial account with us and gain instant access to michigan workers compensation application - which you may then begin using as you wish inside your personal account page. FormsPal guarantees your data privacy by using a protected method that never records or shares any kind of private data involved in the process. Be confident knowing your files are kept safe each time you use our service!