It's quite simple to prepare the ANNUITIES. Our PDF tool was intended to be assist you to fill in any form swiftly. These are the basic steps to follow:
Step 1: Press the "Get Form Now" button to get going.
Step 2: When you have accessed the ANNUITIES editing page you may discover all the actions you can conduct about your document within the upper menu.
The PDF template you desire to fill out will include the next areas:
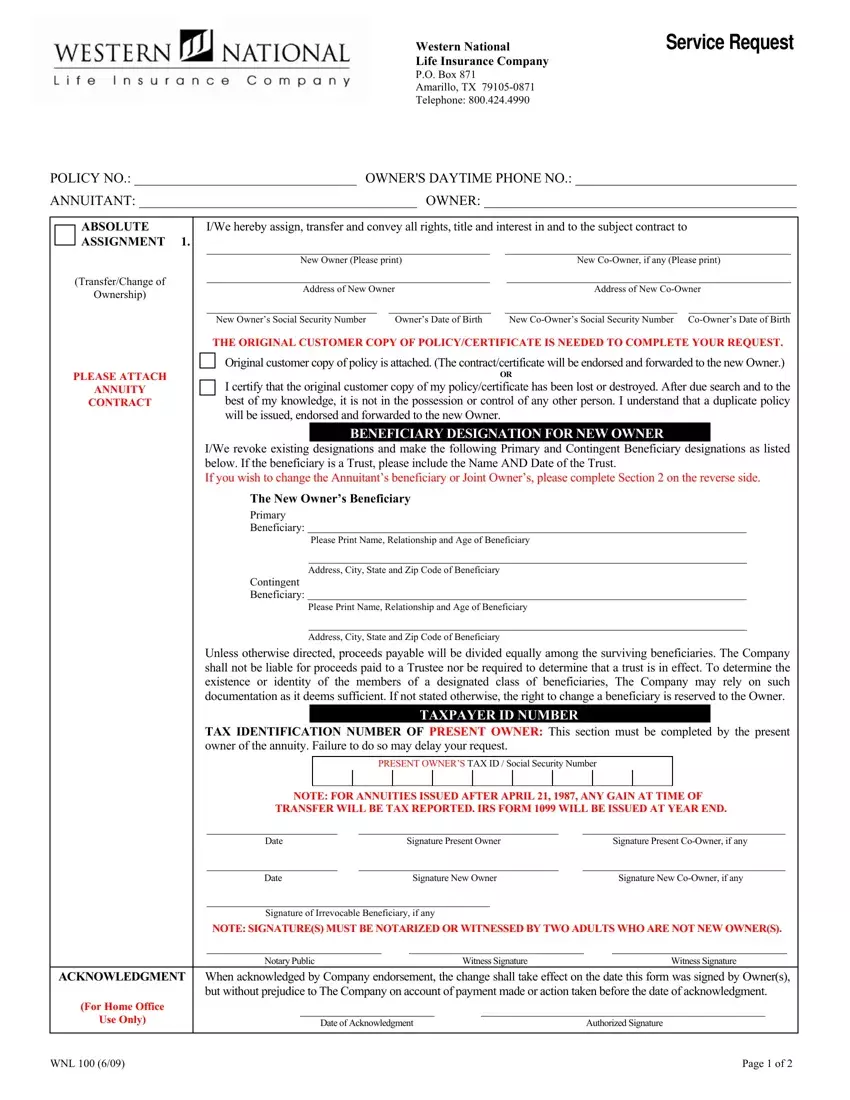
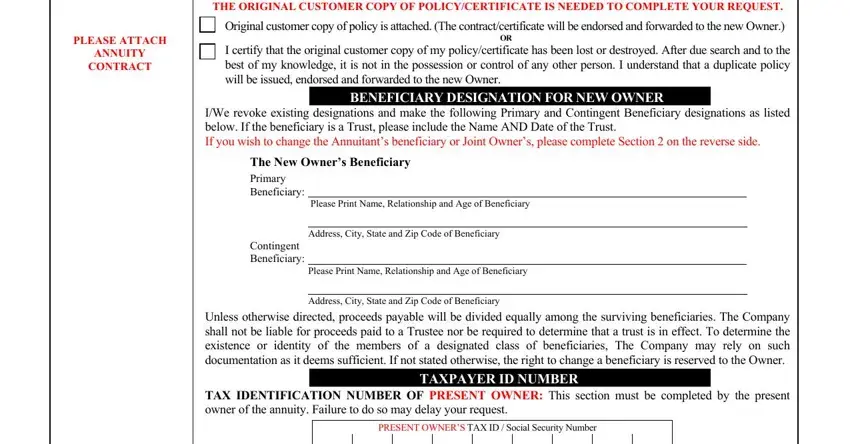
Put down the information in the THE ORIGINAL CUSTOMER COPY OF, Original customer copy of policy, PLEASE ATTACH ANNUITY CONTRACT, BENEFICIARY DESIGNATION FOR NEW, IWe revoke existing designations, The New Owners Beneficiary Primary, Address City State and Zip Code, Address City State and Zip Code, Unless otherwise directed proceeds, and PRESENT OWNERS TAX ID Social field.
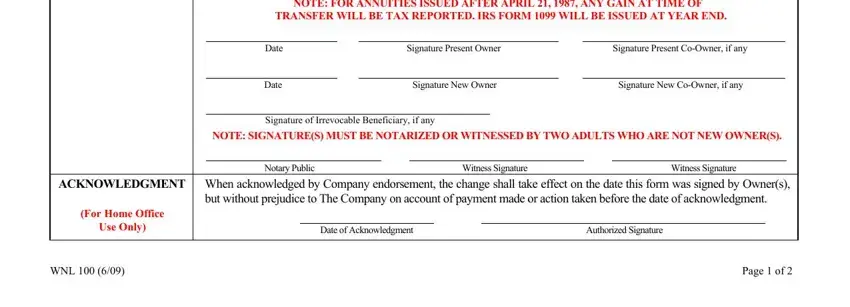
You need to give specific information inside the box NOTE FOR ANNUITIES ISSUED AFTER, Date Signature Present Owner, Date Signature New Owner Signature, Signature of Irrevocable, NOTE SIGNATURES MUST BE NOTARIZED, Notary Public Witness Signature, For Home Office Use Only, but without prejudice to The, Date of Acknowledgment Authorized, WNL, and Page of.
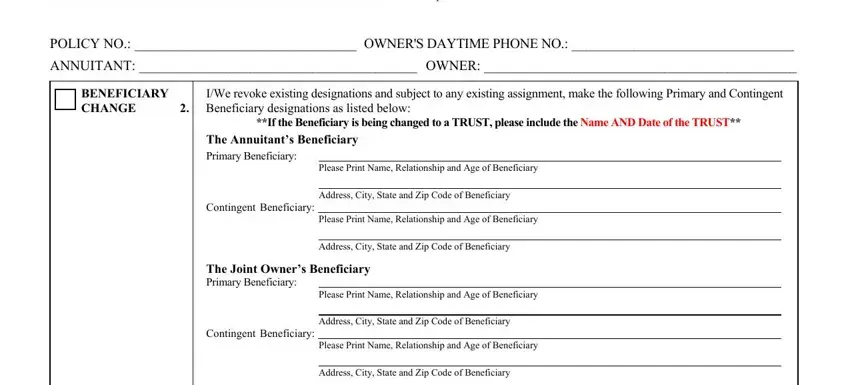
The Western National Life Insurance, POLICY NO OWNERS DAYTIME PHONE NO, BENEFICIARY CHANGE Beneficiary, IWe revoke existing designations, If the Beneficiary is being, The Annuitants Beneficiary Primary, Please Print Name Relationship and, Contingent Beneficiary, Address City State and Zip Code of, Please Print Name Relationship and, Address City State and Zip Code of, The Joint Owners Beneficiary, Please Print Name Relationship and, Contingent Beneficiary, and Address City State and Zip Code of segment should be applied to record the rights or responsibilities of both parties.
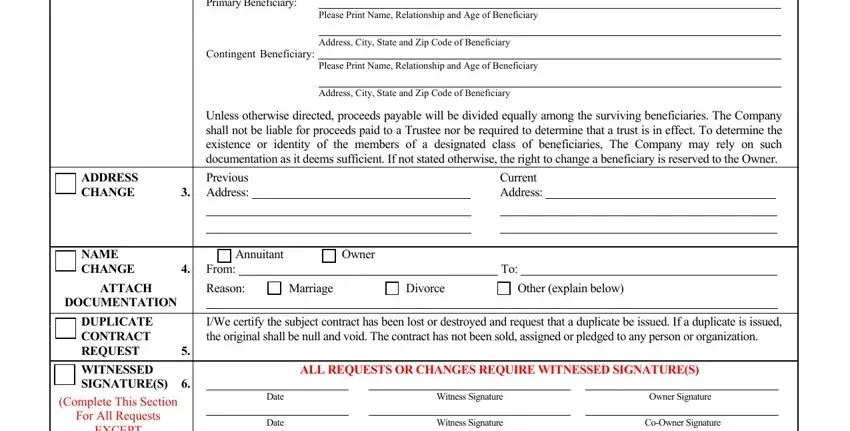
Finalize by looking at the next sections and completing them as required: The Owners Beneficiary Primary, Please Print Name Relationship and, Contingent Beneficiary, Address City State and Zip Code of, Please Print Name Relationship and, Address City State and Zip Code of, Unless otherwise directed proceeds, Previous, Address, Current Address, Annuitant Owner, From To, ADDRESS CHANGE, NAME CHANGE, and ATTACH.
Step 3: Press the Done button to confirm that your finished document is available to be transferred to every device you select or sent to an email you specify.
Step 4: It's going to be safer to create duplicates of the file. You can rest easy that we will not display or see your details.
