Wisconsin Nurse Aide Program
NURSE AIDE REGISTRY RENEWAL FORM INSTRUCTIONS
Federal and state regulations require that you performed nursing or nursing-related services for pay, under the supervision of an RN or LPN, in the past twenty-four (24) months. The Nurse Aide Registry Renewal Form is used to report your nurse aide employment history in order to maintain your eligibility to work in certain federally certified facilities. Failure to re- port your most recent date of employment to the Registry will affect your employment eligibility. The personal informa- tion will be used only to correctly identify and update your Registry records.
Allow two (2) weeks for processing your completed form. To verify the processing status of your Renewal form, you may check your status on the Wisconsin Nurse Aide Registry website at http://www.pearsonvue.com or call the Wisconsin Nurse Aide Registry at (877) 329-8760.
If you are on active military duty when your certification expires, or if you are the civilian spouse of a service member on active military duty when your certification expires and are unable to practice under your nurse aide certification during your spouse’s active military duty, you may be eligible for an extension of your certification for 180 days after the date of discharge from active duty and to renew your certification to the next biennium without completing the required re-testing. For information on how to renew your certification, please contact the Office of Caregiver Quality at (608) 261-8319 or DHSCaregiverIntake@wi.gov.
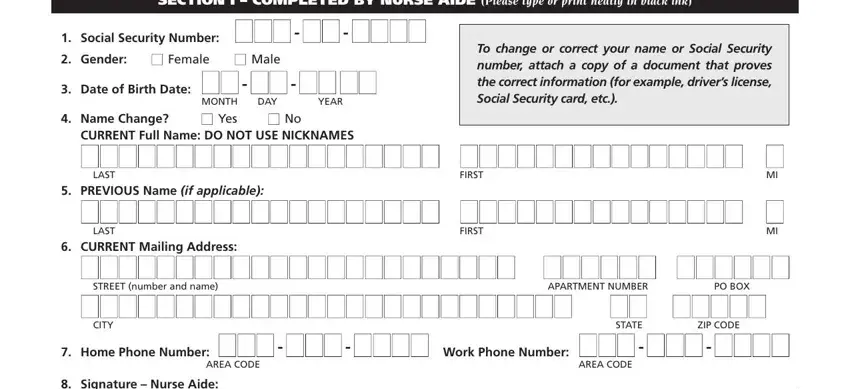
SECTION I — COMPLETED BY THE NURSE AIDE
1.Social Security number: Enter your Social Security number or previously assigned Nurse Aide Registry identification number. Providing your Social Security number is voluntary. Social Security numbers are used to determine nurse aide employment eligibility for prospective employers.
2.Gender: Check the appropriate box, female or male.
3.Date of Birth: Enter your month, date, and year of birth.
4.Current Legal Name: Check “yes” if your name has changed. Enter your current full name (last, first, and middle initial). Do NOT use nicknames (for example, enter “William” instead of “Bill”, “Jennifer” instead of “Jenny”, “Richard” instead of “Dick”, etc.).
5.Previous Name (if applicable): Enter your previous name if any change in your last name, first name, or middle initial has oc- curred (for example, maiden name, name change, etc.).
To change or correct your name or Social Security number, attach a copy of a document that proves the correct informa- tion (for example, driver’s license, Social Security card, etc.).
6.Current Mailing Address: Enter your current address (street, P.O. box, city, state, and ZIP).
7.Home/Work Telephone Number: Enter your current home and work telephone numbers.
8.Nurse Aide Signature: Sign and date the form.
SECTION II — COMPLETED BY THE HEALTH CARE EMPLOYER
9.Enter the individual’s starting date of employment at your facility.
10.Check “Yes” or “No” if the nurse aide has provided nurse aide services for at least eight (8) hours for pay during the twenty-four (24) months before their registration expiration date. If yes, enter the date the individual most recently worked as a nurse aide in a nursing-related service. Paid work in the following direct patient care settings under the supervision of an RN or LPN may be considered. If the nursing-related work setting is not listed below, and you feel it should count for renewal on the Wisconsin Nurse Aide Registry, enter the name and the type of health care facility.
11.Current or most recent health care employer: Enter the name, type of health care facility, full address, and telephone number of the facility. Indicate whether the nurse aide is your direct employee or a contracted pool aide.
12.Signature of facility representative: A representative of the health care facility must sign his/her name and date the form, verifying that an RN or LPN is supervising the nurse aide’s nursing-related duties. Please note that if the individual is employed by a temporary or pool agency, a representative of the health care facility, not of the temporary or pool agency, must complete this section.
Mail the COMPLETED form to:
Pearson VUE – Wisconsin Nurse Aide Registry
PO Box 13785
Philadelphia, PA 19101-3785