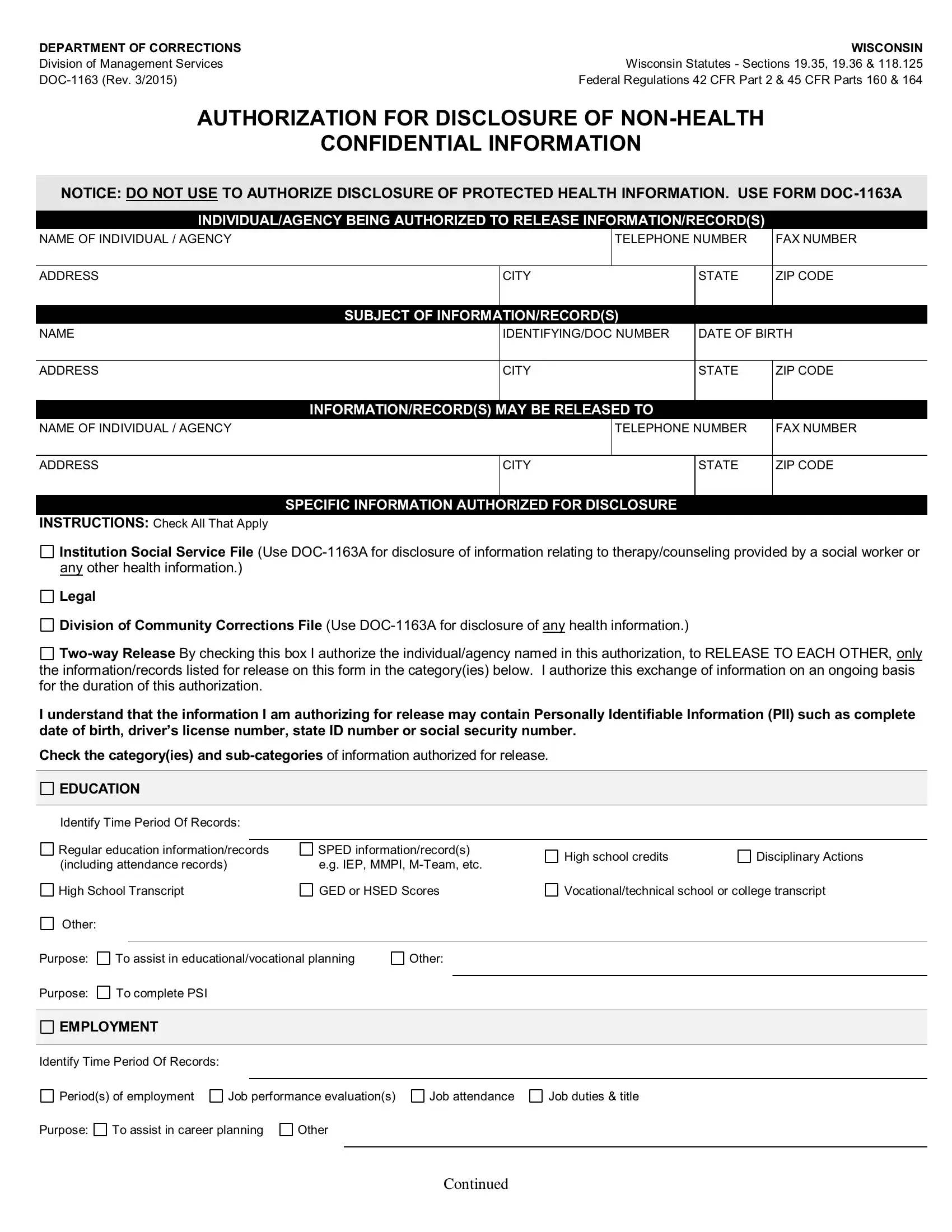
In the complex landscape of legal and personal record sharing, the Wisconsin Department of Corrections provides a structured means via the Wisconsin Doc 1163 form. This document serves a pivotal role by authorizing the release of non-health confidential information under specific regulatory umbrellas including the Wisconsin Statutes - Sections 19.35, 19.36 & 118.125, alongside federal regulations outlined in 42 CFR Part 2 & 45 CFR Parts 160 & 164. It distinguishes itself by prohibiting the use for health information disclosure, directing such needs to form DOC-1163A instead. The form meticulously defines the spectrum of information that can be disclosed, spanning educational achievements, employment history, and disciplinary actions, yet emphasizes the protection of personally identifiable information (PII). It underscores the rights of individuals regarding the authorization process, the conditions under re-disclosure laws, and the time frame of the authorization's validity. Through checkboxes and specified fields, it facilitates a tailored authorization that resonates with the individual's intentions, whether for educational/vocational planning, employment verification, or legal requirements. Signature blocks and directives ensure that the authorization accurately reflects the wishes of the individual, underscoring the importance of informed consent in the release of confidential records.
| Question | Answer |
|---|---|
| Form Name | Wisconsin Doc 1163 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | department of corrections forms, wi doc non health online, wi authorization confidential information printable, wisconsin doc authorization confidential |
DEPARTMENT OF CORRECTIONS |
WISCONSIN |
|
Division of Management Services |
Wisconsin Statutes - Sections 19.35, 19.36 |
& 118.125 |
Federal Regulations 42 CFR Part 2 & 45 CFR Parts |
160 & 164 |
|
AUTHORIZATION FOR DISCLOSURE OF
CONFIDENTIAL INFORMATION
NOTICE: DO NOT USE TO AUTHORIZE DISCLOSURE OF PROTECTED HEALTH INFORMATION. USE FORM
INDIVIDUAL/AGENCY BEING AUTHORIZED TO RELEASE INFORMATION/RECORD(S)
NAME OF INDIVIDUAL / AGENCY |
|
|
TELEPHONE NUMBER |
FAX NUMBER |
|
|
|
|
|
|
|
ADDRESS |
|
CITY |
STATE |
ZIP CODE |
|
|
|
|
|
|
|
|
SUBJECT OF INFORMATION/RECORD(S) |
|
|
||
NAME
ADDRESS
IDENTIFYING/DOC NUMBER |
DATE OF BIRTH |
||
CITY |
STATE |
|
ZIP CODE |
|
|||
|
|
|
|
INFORMATION/RECORD(S) MAY BE RELEASED TO
NAME OF INDIVIDUAL / AGENCY |
|
TELEPHONE NUMBER |
FAX NUMBER |
|
|
|
|
|
|
ADDRESS |
CITY |
|
STATE |
ZIP CODE |
|
|
|
|
|
SPECIFIC INFORMATION AUTHORIZED FOR DISCLOSURE
INSTRUCTIONS: Check All That Apply
Institution Social Service File (Use
Legal
Division of Community Corrections File (Use
I understand that the information I am authorizing for release may contain Personally Identifiable Information (PII) such as complete date of birth, driver’s license number, state ID number or social security number.
Check the category(ies) and
EDUCATION
Identify Time Period Of Records:
Regular education information/records (including attendance records)
High School Transcript
Other:
SPED information/record(s) e.g. IEP, MMPI,
GED or HSED Scores
High school credits |
Disciplinary Actions |
Vocational/technical school or college transcript
Purpose: To assist in educational/vocational planning
Purpose: To complete PSI
Other:
EMPLOYMENT
Identify Time Period Of Records: |
|
|
|
Period(s) of employment |
Job performance evaluation(s) |
||
Purpose: |
To assist in career planning |
Other |
|
Job attendance
Job duties & title
CONTINUED
Purpose: |
To complete PSI |
|
|
OTHER
Identify Time Period Of Records:
Type(s) or information/record(s):
Purpose:
YOUR RIGHTS WITH RESPECT TO THIS AUTHORIZATION
Signing of Authorization - I am under no legal obligation to sign this authorization. If I do, I have a right to receive a copy.
AODA Information - My educational information/record(s) may contain alcohol and other drug abuse information. If so, I must sign
Right to Inspect and/or Copy Education Information/Records - I have the right to inspect and copy my educational records as permitted under s. 118.125 Wis. Stats. I may be charged a reasonable fee for copies.
|
|
AUTHORIZATION SIGNATURE |
INITIAL ONE ONLY (Required) |
|
|
|
Authorization expires as of: |
, (Date) |
|
||
|
Authorization expires: |
, month(s) from the date I sign this authorization. |
|
||
Authorization expires after the following action takes place:
Authorization expires upon substantial change in criminal justice system status. (e.g., released from prison.)
If no date/event is entered, this Authorization expires one year from the date of signing.
I have read or had read to me the contents of this authorization. I have had an opportunity to discuss and ask questions. By signing this authorization, I am confirming that it accurately reflects my wishes regarding disclosure of confidential information.
SIGNATURE OF INDIVIDUAL WHO IS SUBJECT OF RECORD |
|
DATE SIGNED |
|
|
|
SIGNATURE OF OTHER PERSON LEGALLY AUTHORIZED |
TITLE OR RELATIONSHIP TO INDIVIDUAL WHO IS |
DATE SIGNED |
TO CONSENT TO DISCLOSURE (If Applicable) |
SUBJECT OF RECORD |
|
|
|
|
FAX OR PHOTOCOPY MAY BE TREATED AS ORIGINAL
DISTRIBUTION: Original- Individual/Agency authorized to release Information/Record(s);
Official