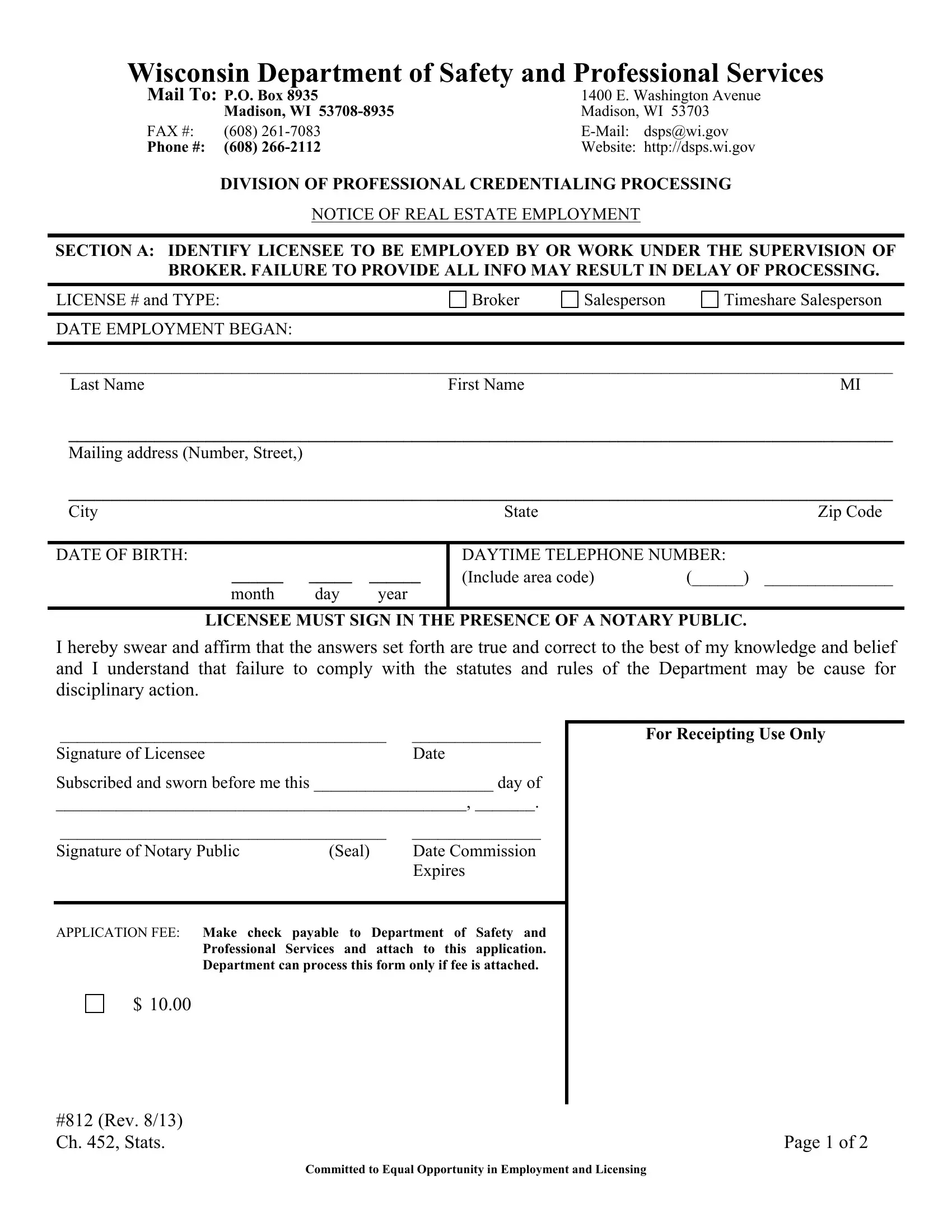
In the complex realm of real estate employment in Wisconsin, the Form 812 emerges as a pivotal document, underlining the imperative connection between real estate licensees and their brokers. Administered by the Wisconsin Department of Safety and Professional Services, this form serves a crucial role in the professional credentialing process, ensuring that all real estate employment arrangements are officially recorded and acknowledged by the state's regulatory framework. It meticulously collects details about the licensee, including their license type—whether they are a broker, salesperson, or timeshare salesperson—and the exact date employment began. Essential identification information such as name, mailing address, date of birth, and contact numbers are also part of the requisites, alongside the mandatory notarization of the licensee's signature to attest to the veracity of the information provided. A significant section of this form is also dedicated to identifying the broker or employing entity, requiring detailed data about the broker-employer, including their license type and main office address. This segment ensures that the broker assumes responsibility for the licensee, a measure that underscores the seriousness of professional conduct and adherence to statutory regulations and rules of the Department. This form, updated in August 2013, further emphasizes the Department of Safety and Professional Services' commitment to equal opportunity in employment and licensing, marking a $10 application fee that accompanies the process. Through its comprehensive structure, the Wisconsin 812 Form not only facilitates smooth employment processes but also fortifies the regulatory framework that upholds the integrity of the real estate profession within the state.
| Question | Answer |
|---|---|
| Form Name | Wisconsin Form 812 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | fm812 form 812 notice of real estate employment |
Wisconsin Department of Safety and Professional Services
Mail To: P.O. Box 8935 |
1400 E. Washington Avenue |
||
|
Madison, WI |
Madison, WI 53703 |
|
FAX #: |
(608) |
dsps@wi.gov |
|
Phone #: |
(608) |
Website: |
http://dsps.wi.gov |
DIVISION OF PROFESSIONAL CREDENTIALING PROCESSING
NOTICE OF REAL ESTATE EMPLOYMENT
SECTION A: IDENTIFY LICENSEE TO BE EMPLOYED BY OR WORK UNDER THE SUPERVISION OF BROKER. FAILURE TO PROVIDE ALL INFO MAY RESULT IN DELAY OF PROCESSING.
LICENSE # and TYPE: |
Broker |
Salesperson |
Timeshare Salesperson |
|
|
|
|
DATE EMPLOYMENT BEGAN: |
|
|
|
|
|
|
|
_________________________________________________________________________________________________
Last NameFirst NameMI
________________________________________________________________________________________________
Mailing address (Number, Street,)
________________________________________________________________________________________________
City |
State |
Zip Code |
DATE OF BIRTH:
______ _____ ______
month day year
DAYTIME TELEPHONE NUMBER:
(Include area code) |
(______) _______________ |
LICENSEE MUST SIGN IN THE PRESENCE OF A NOTARY PUBLIC.
I hereby swear and affirm that the answers set forth are true and correct to the best of my knowledge and belief and I understand that failure to comply with the statutes and rules of the Department may be cause for disciplinary action.
______________________________________ |
_______________ |
Signature of Licensee |
Date |
Subscribed and sworn before me this _____________________ day of
________________________________________________, _______.
______________________________________ |
_______________ |
|
Signature of Notary Public |
(Seal) |
Date Commission |
|
|
Expires |
APPLICATION FEE: Make check payable to Department of Safety and
Professional Services and attach to this application. Department can process this form only if fee is attached.
For Receipting Use Only
$ 10.00
#812 (Rev. 8/13) |
|
Ch. 452, Stats. |
Page 1 of 2 |
Committed to Equal Opportunity in Employment and Licensing
Wisconsin Department of Safety and Professional Services
SECTION B: THIS SECTION IDENTIFIES THE BROKER WITH WHOM OR BY WHOM THE
LICENSEE IN SECTION A WILL BE ASSOCIATED OR EMPLOYED
TYPE OF LICENSE: |
Sole Proprietor Broker
Business Entity (Association, LLC, LLP)
PRINT NAME AND ADDRESS OF
_________________________________________________________________________________________________
Business Entity Name
_________________________________________________________________________________________________
Business Address of
_____________________________________________ |
(_____) ______________________________________ |
License Number: |
Main Office Telephone Number: |
This statement must be signed by the sole proprietor
This is to certify that the
_________________________________________________________
Print name of person signing below |
|
_________________________________________________________ |
________________________ |
Signature of either the sole proprietor broker or a director, manager, |
Date |
member, officer, owner or partner of the licensed business |
|
entity listed above. |
|
|
|
#812 (Rev. 8/13) |
|
Ch. 452, Stats. |
Page 2 of 2 |
Committed to Equal Opportunity in Employment and Licensing