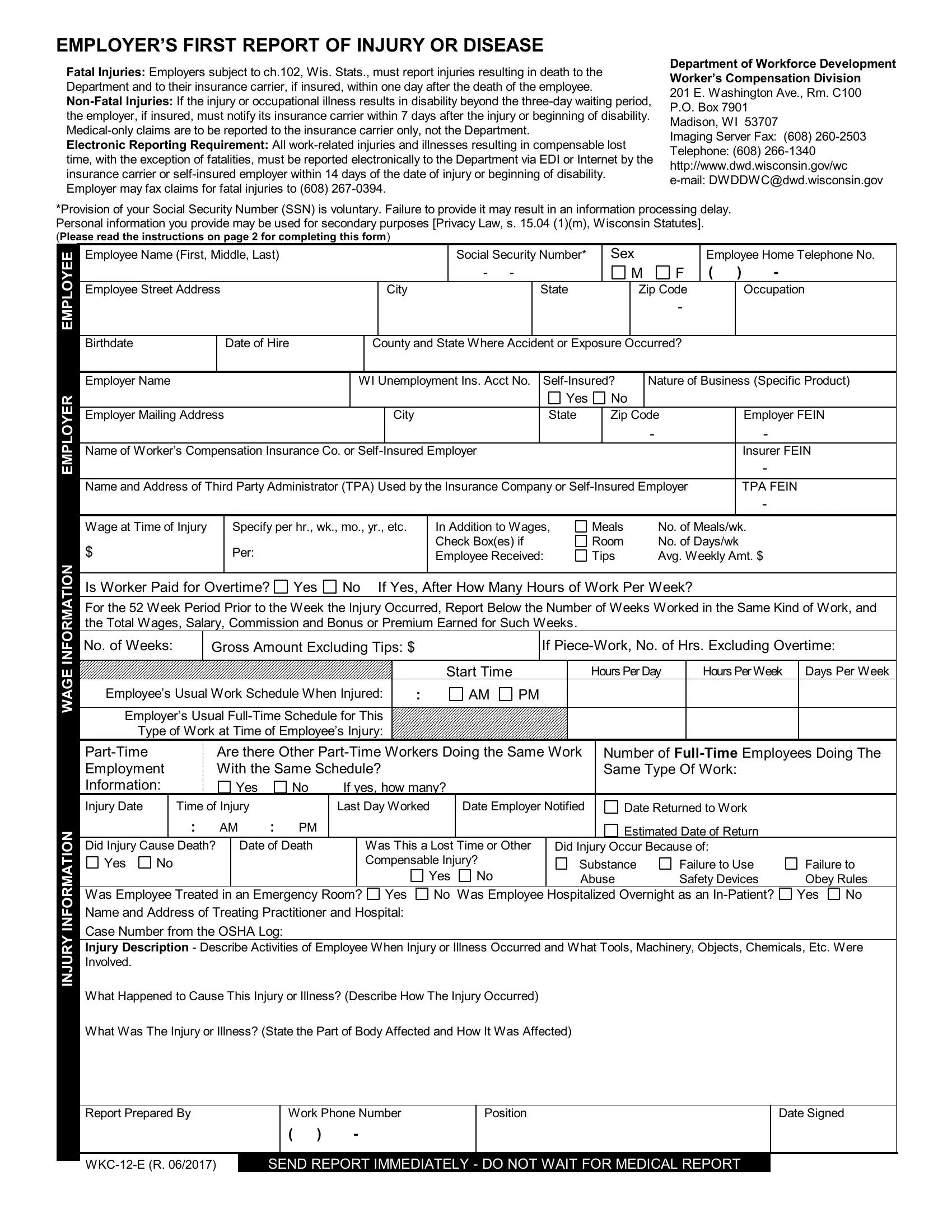
In the realm of occupational safety and health, the WKC-12E form serves as a critical tool for employers to report work-related injuries or diseases, a necessity underscored by its detailed requirements and procedural directives. This form, mandated by the Wisconsin Department of Workforce Development's Worker’s Compensation Division, imposes specific deadlines for reporting both fatal and non-fatal incidents to ensure timely communication between employers, insurance carriers, and the state. For fatal injuries, the form necessitates submission within a day, demonstrating the urgency attributed to such grave circumstances. Non-fatal injuries that surpass a three-day waiting period, conversely, initiate a different protocol, requiring notification within seven days if the incident results in disability, and stipulating an electronic submission method for most reports to streamline and expedite the process. Additional nuances include stipulations for reporting wages, employee information, and details surrounding the injury or disease -- all designed to nurture a comprehensive understanding of each incident. Remarkably, the WKC-12E form also aligns with the Occupational Safety and Health Administration's (OSHA) reporting guidelines, allowing employers to satisfy federal requirements concurrently, illustrating its role not just as a bureaucratic necessity but as a scaffold supporting both state and federal worker safety initiatives.
| Question | Answer |
|---|---|
| Form Name | Wkc 12 E Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | wisconsin disease dwd, wi wkc workforce development, wi wkc dwd workforce, wi employers injury dwd |
EMPLOYER’S FIRST REPORT OF INJURY OR DISEASE
Fatal Injuries: Employers subject to ch.102, Wis. Stats., must report injuries resulting in death to the Department and to their insurance carrier, if insured, within one day after the death of the employee.
Electronic Reporting Requirement: All
Department of Workforce Development
Worker’s Compensation Division
201 E. Washington Ave., Rm. C100 P.O. Box 7901
Madison, WI 53707
Imaging Server Fax: (608)
Telephone: (608)
*Provision of your Social Security Number (SSN) is voluntary. Failure to provide it may result in an information processing delay. Personal information you provide may be used for secondary purposes [Privacy Law, s. 15.04 (1)(m), Wisconsin Statutes].
(Please read the instructions on page 2 for completing this form)
EMPLOYER EMPLOYEE
WAGE INFORMATION
INJURY INFORMATION
Employee Name (First, Middle, Last) |
|
|
|
|
|
|
|
Social Security Number* |
|
Sex |
|
Employee Home Telephone No. |
||||||||
|
|
|
|
|
|
|
|
|
|
- |
- |
|
|
|
|
M |
F |
( |
) |
- |
Employee Street Address |
|
|
|
|
|
|
City |
|
|
|
|
State |
|
|
Zip Code |
|
|
Occupation |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Birthdate |
|
Date of Hire |
|
|
|
County and State Where Accident or Exposure Occurred? |
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||
Employer Name |
|
|
|
WI Unemployment Ins. Acct No. |
Nature of Business (Specific Product) |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
No |
|
|
|
|
|
Employer Mailing Address |
|
|
|
|
|
|
City |
|
|
|
|
State |
|
Zip Code |
|
|
Employer FEIN |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
- |
|
|
- |
Name of Worker’s Compensation Insurance Co. or Self- |
Insured Employer |
|
|
|
|
|
|
|
|
|
Insurer FEIN |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
- |
Name and Address of Third Party Administrator (TPA) Used by the Insurance Company or |
|
|
TPA FEIN |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
- |
|
|
|
|
|
|
|||||||||||||||
Wage at Time of Injury |
Specify per hr., wk., mo., yr., etc. |
In Addition to Wages, |
Meals |
No. of Meals/wk. |
||||||||||||||||
$ |
|
Per: |
|
|
|
|
|
|
Check Box(es) if |
Room |
No. of Days/wk |
|
||||||||
|
|
|
|
|
|
|
Employee Received: |
Tips |
Avg. Weekly Amt. $ |
|||||||||||
|
|
|
|
|
|
|
|
|||||||||||||
Is Worker Paid for Overtime? |
Yes |
No If Yes, After How Many Hours of Work Per Week? |
|
|
|
|||||||||||||||
For the 52 Week Period Prior to the Week the Injury Occurred, Report Below the Number of Weeks Worked in the Same Kind of Work, and the Total Wages, Salary, Commission and Bonus or Premium Earned for Such Weeks.
No. of Weeks: |
|
Gross Amount Excluding Tips: $ |
|
|
|
If |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
Start Time |
|
|
|
Hours Per Day |
|
Hours Per Week |
|
Days Per Week |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Employee’s Usual Work Schedule When Injured: |
|
: |
AM |
PM |
|
|
|
|
|
|
|
|
|
|||||||||
Employer’s Usual |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Type of Work at Time of Employee’s Injury: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
Are there Other |
Number of |
||||||||||||||||||
Employment |
|
|
With the Same Schedule? |
|
|
|
|
|
Same Type Of Work: |
|
|
|||||||||||
Information: |
|
|
|
Yes |
|
|
No |
If yes, how many? |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Injury Date |
|
Time of Injury |
|
|
|
Last Day Worked |
Date Employer Notified |
|
|
Date Returned to Work |
|
|
||||||||||
|
|
: |
|
AM |
: PM |
|
|
|
|
|
|
|
|
|
Estimated Date of Return |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Did Injury Cause Death? |
|
Date of Death |
Was This a Lost Time or Other |
Did Injury Occur Because of: |
|
|
||||||||||||||||
Yes |
No |
|
|
|
|
|
|
|
Compensable Injury? |
|
|
Substance |
Failure to Use |
|
Failure to |
|||||||
|
|
|
|
|
|
|
|
|
|
|
Yes |
No |
|
|
Abuse |
Safety Devices |
|
Obey Rules |
||||
Was Employee Treated in an Emergency Room? Yes No Was Employee Hospitalized Overnight as an
Case Number from the OSHA Log:
Injury Description - Describe Activities of Employee When Injury or Illness Occurred and What Tools, Machinery, Objects, Chemicals, Etc. Were Involved.
What Happened to Cause This Injury or Illness? (Describe How The Injury Occurred)
What Was The Injury or Illness? (State the Part of Body Affected and How It Was Affected)
Report Prepared By |
Work Phone Number |
Position |
Date Signed |
|
|
( ) |
- |
|
|
|
|
|
||
SEND REPORT IMMEDIATELY - DO NOT WAIT FOR MEDICAL REPORT |
|
|||
EMPLOYER AND INSURANCE CARRIER INSTRUCTIONS
The employer must complete all relevant sections on this form and submit it to the employer’s worker’s compensation insurance carrier or third party claim administrator within seven (7) days after the date of a
used to immediately report any injury requiring medical treatment, even though it does not involve lost work time.
For any work injury resulting in a fatality, the employer must also submit this form directly to the Department of Workforce Development within 24 hours of the fatality.
An employer exempt from the duty to insure under s. 102.28, Wis. Stats., and an insurance carrier administering claims for an insured employer are required to submit this form to the Department of Workforce Development within 14 days of the date of work injury.
MANDATORY INFORMATION
In order to accurately administer claims, each of the following sections of this form must be completed. The First Report of Injury will be returned to the sender if the mandatory information is not provided.
Employee Section: Provide all requested information to identify the injured employee. If an employee has multiple dates of employment, the “Date of Hire” is the date the employee was hired for the job on which he or
she was injured.
Employer Section: Provide all requested information to identify the injured worker’s employer at the time of
injury. Provide the name and Federal Employer Identification Number (FEIN) for the insurance carrier or self- insured employer responsible for the worker’s compensation expenses for this injury. Also identify the third
party claim administrator, if one is used for this claim.
Wage Information Section: Provide the information requested regarding the injured employee’s wage and hours worked for the job being performed at the time of injury.
Injury Information Section: Provide information regarding the date and time of injury. Provide a detailed description of the injury, including part of the body injured, the specific nature of the injury (i.e., fracture, strain, concussion, burn, etc.) and the use of any objects or tools (i.e., saw, ladder, vehicle, etc.) that may have caused the injury. Provide the name of the person preparing this report and the telephone number at which they may be reached, if additional information is needed. This form was designed to include information required by OSHA on form 301. If this section is completed and retained, the employer will not have to complete the OSHA 301 form.