It is really straightforward to complete the workers comp designated provider letter spaces. Our tool will make it virtually effortless to work with any specific PDF file. Down the page are the primary four steps you need to take:
Step 1: The initial step requires you to choose the orange "Get Form Now" button.
Step 2: As soon as you've accessed the editing page workers comp designated provider letter, you will be able to discover each of the options readily available for the document at the upper menu.
These sections will make up the PDF document that you will be filling out:
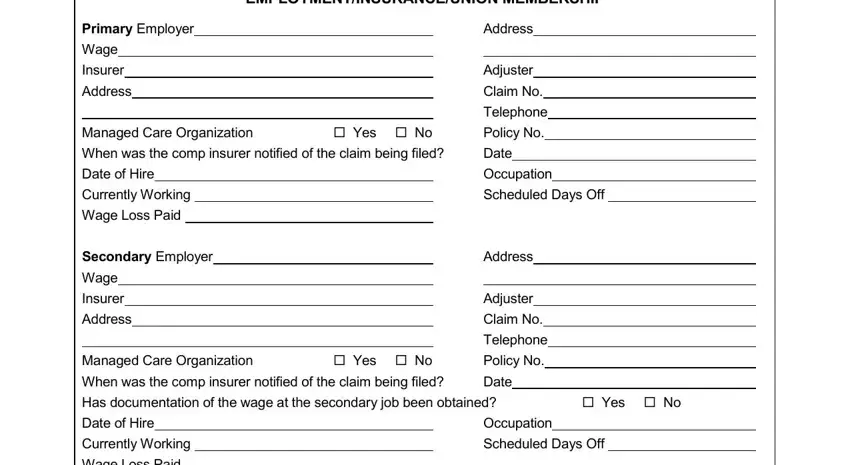
Complete the EMPLOYMENTINSURANCEUNION MEMBERSHIP, Primary Employer, Wage, Insurer, Address, Managed Care Organization When was, Yes No, Date of Hire Currently Working, Wage Loss Paid, Secondary Employer, Wage Insurer, Address, Managed Care Organization, Yes No, and Address fields with any information that are requested by the system.
The system will ask you for details to conveniently submit the area NonIndustrial Carrier, Yes No, Policy No, Carrier Address, Private Health Carrier if any, Yes No, Policy No, Carrier, Address, Union Membership Union Name, Date of Injury WCB No, Body Parts Injured, How Did the Injury Occur, Yes No, and Local No.
The Where Did the Injury Occur, PRIOR CLAIMS, Date of Prior Workers Comp Claim, Amount of Award, Amount of Award, and PREVIOUS MOTOR VEHICLE ACCIDENTS section could be used to indicate the rights and responsibilities of both parties.
Check the sections MEDICAL CONDITIONS PREEXISTING, PRIOR ARRESTS AND CONVICTIONS, and MENTAL HEALTH ALCOHOL DRUG USE and next complete them.
Step 3: If you're done, click the "Done" button to export your PDF document.
Step 4: In order to prevent possible forthcoming complications, take the time to have up to several copies of any form.
