USCIS Form N-648, officially titled “Medical Certification for Disability Exceptions,” is used by applicants for U.S. citizenship who seek an exception to the English and civics testing requirements for naturalization due to physical or developmental disabilities or mental impairments. The form must be completed by a licensed medical doctor, doctor of osteopathy, or clinical psychologist. It requires detailed information about the nature and extent of the applicant’s disability and how it impairs their ability to meet the testing requirements for citizenship.
Other USCIS Forms
Look through some related IRS forms that wage earners and self-employed individuals might find useful.
For your comfort, we created the form-building software that you can utilize to fill the Form N-648. By utilizing our platform for legal forms editing, you can be sure you won’t miss anything while completing the form.
Write down the full name and full address (including city, street name and number, country, postal code, etc.) of the candidate.

Fill in the candidate’s birth date, phone number, email, gender, and security number.
Write down the medical worker’s data, including full legal name, physical address (containing the city, street name, and number, country, postal code), license number, Email, daytime contact phone number, the medical worker’s category, type of medical practice.

Give detailed data on the candidate’s incapacities. Indicate when each of the incapacities began. Write down the grounds of the incapacities. Ensure to mention through which medical methods the incapacities were diagnosed. Indicate the incapacities severity. Describe how the incapacities affect the candidate’s everyday life. Indicate if any of the incapacities will last for the next 12 months and why. Answer if any of the candidate’s incapacities were caused by the use of drugs. Describe in which way the incapacities of the candidate affect his impossibility to prove the English language proficiency and how they stop him or her from meeting the civics demands. Indicate the date when the incapacity was first examined.



Write down the date and location where the candidate’s incapacities were examined in the first place. Make sure to mention the city, street number, postal code and zip code, date of the incapacities’ examination.
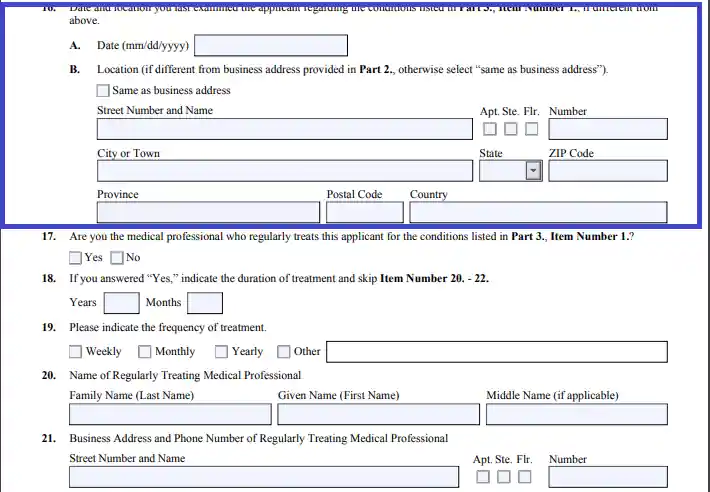
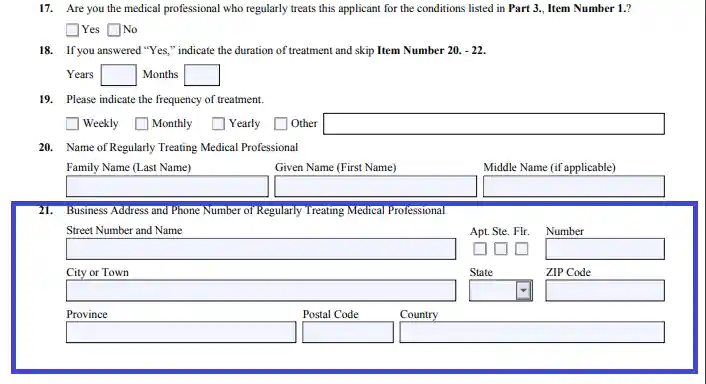
Indicate the duration of the candidate’s treatment, give detailed data on its frequency, and fill in the medical worker’s full name for treating the candidate. Fill in the full business address of the subject medical worker, including the city, street number, postal code, and ZIP.
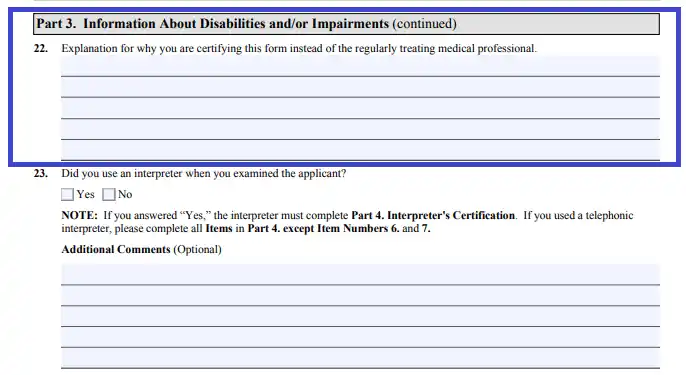
Explain the necessity of this form completion instead of treating the candidate’s incapacities. Indicate if you were using an interpreter while signing the form.
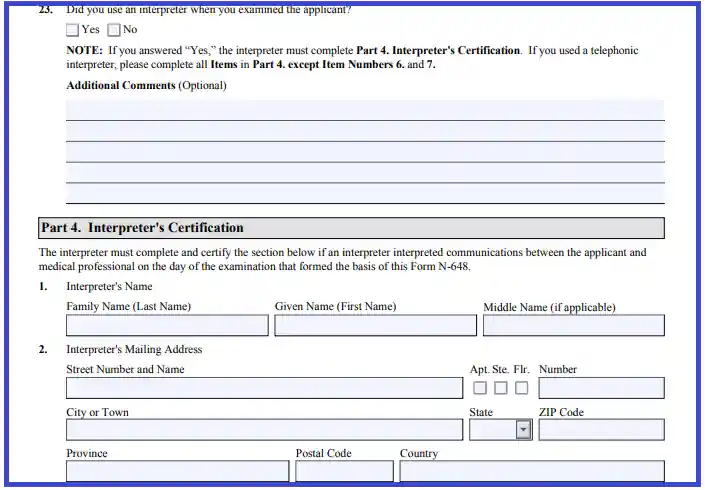
If an interpreter took part in the form completion, fill in the form his or her full name, full address (including the city, street number, postal code, and zip code), email, and phone number.
Supply an interpreter’s sign and the form completion date. Also, in this section of the form, you need to indicate if the telephonic interpreter participated in the form completion, and if so, give some information regarding the topic.


A candidate has to write down their full name, the name of the verified medical worker, sign the completed form, and, finally, fill in the form completion date.
Indicate if an interpreter was a participant in the form completion. If not, fill in the reasoning for this. Choose the correct identity document by which the candidate was identified.
A certified medical worker has to sign the completed form and fill in the form completion date.