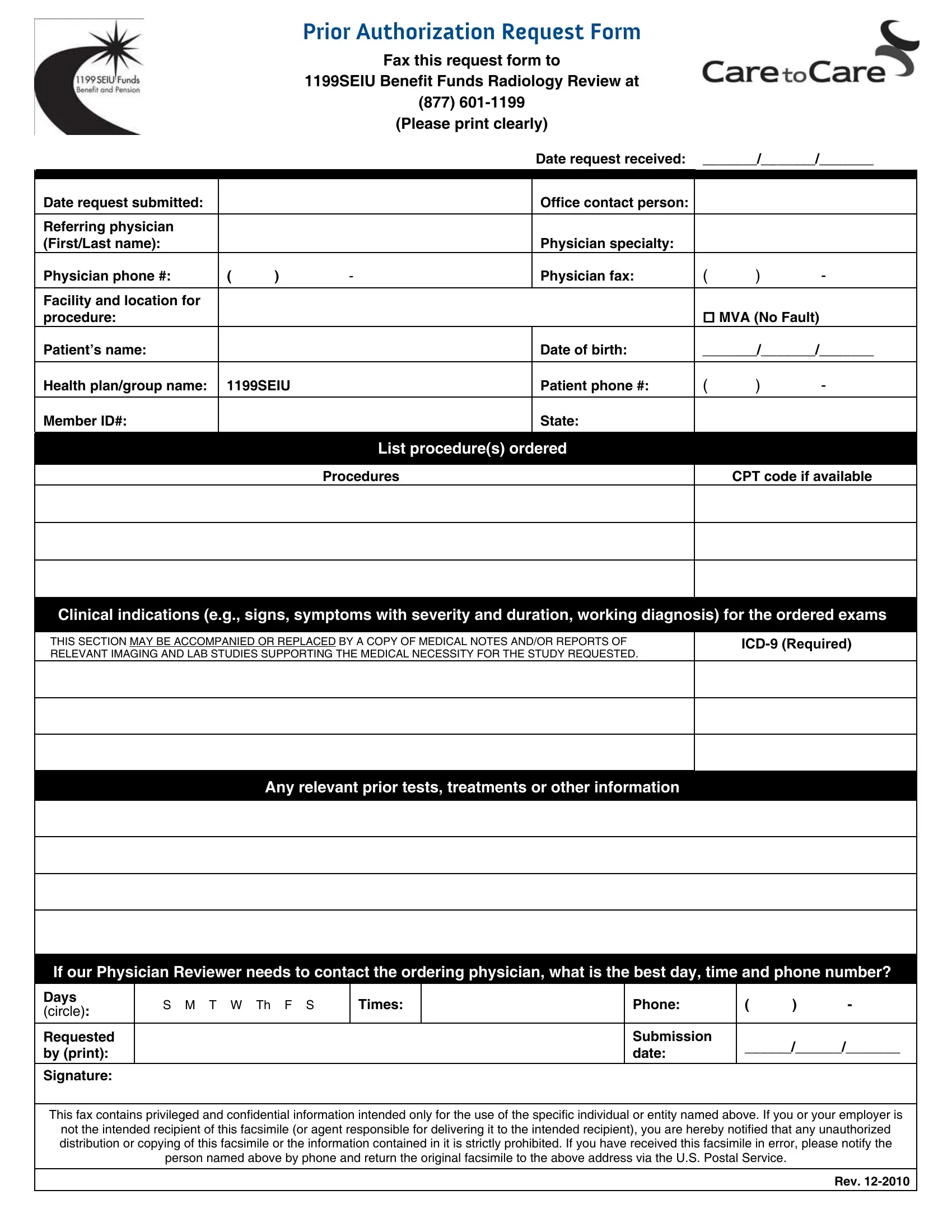

The 1199 Authorization Form must be completed accurately and faxed to the 1199SEIU Benefit Funds to obtain prior authorization for radiology procedures. Work through each section in order to avoid delays or denials. FormsPal's PDF editor lets you type directly into the form before printing and faxing.
Step 1: Record the Date and Office Contact Information
Write the date of the request at the top of the form. Enter the office contact name, direct phone number, and fax number. This information allows the physician reviewer to follow up with your office quickly if additional clinical details are needed to complete the review.
Step 2: Enter the Referring Physician Details
Provide the full name of the ordering physician along with the office address. Enter the physician's preferred callback time and hours of availability. The reviewer may call the ordering provider directly to discuss clinical findings, so current and accurate contact information is critical to a smooth review process.
Step 3: Complete the Patient Information Section
Record the patient's full legal name and date of birth. Enter the patient's 1199SEIU member ID number exactly as shown on their benefit fund ID card. Include the health plan or group name. Errors in the member ID or date of birth are among the most common reasons for authorization delays, so verify these fields carefully before faxing.
Step 4: List the Requested Procedures and Codes
Identify each imaging procedure being requested by full name and include the corresponding CPT code. Enter ICD-10 diagnosis codes that support the clinical indication for each exam. The form provides space for multiple procedures, so list all studies requiring authorization in a single submission.
Step 5: Describe Clinical Indications and Supporting Evidence
Use this section to explain why each imaging procedure is medically necessary. Describe the patient's symptoms, physical examination findings, and any prior diagnostic tests already performed. Specific and detailed clinical information speeds up the review process and reduces the chance of denial. Attach supporting records or notes to the fax when available.
Step 6: Fax the Completed Form to 1199SEIU
Once all sections are completed, fax the form to the 1199SEIU Benefit Funds number printed on the form cover. Retain a copy in the patient's file for reference. If you do not receive a response within two business days, follow up directly with the fund to check the status of the request.
What Is the 1199 Authorization Form Used For?
The 1199 Authorization Form is used to obtain prior authorization for radiology and advanced imaging procedures covered by the 1199SEIU Benefit Funds. The fund requires prior authorization for studies such as MRI, CT scans, PET scans, ultrasound, and other high-cost imaging before the patient receives care. Submitting the form in advance ensures the procedure will be covered under the member's benefit plan.
The 1199SEIU Benefit Funds provide health coverage for union members and their dependents employed in the healthcare, long-term care, and home care industries across New York and several other states. Providers must submit prior authorization before scheduling most imaging procedures. Procedures performed without prior authorization may not be eligible for reimbursement.
If the patient's insurance is not through 1199SEIU, other authorization forms may apply. Review the patient's insurance card or contact the insurer directly to confirm the correct form and submission process.
Frequently Asked Questions
What information is required to complete the 1199 Authorization Form?
The form requires the patient's full name, date of birth, and 1199SEIU member ID. Providers must also include the referring physician's name and contact details, CPT codes for each requested imaging study, ICD-10 diagnosis codes, and a written description of the clinical indications. All fields marked as required must be completed for the form to be processed without delay.
How long does the 1199 authorization review take?
Most prior authorization requests submitted with complete information are reviewed within two to five business days. Requests with missing or unclear information may take longer or be returned for correction. Providers requesting urgent authorization should contact the 1199SEIU Benefit Funds directly to ask about expedited review options.
What should I do if the authorization request is denied?
If the 1199 Authorization Form request is denied, the provider can submit additional clinical documentation to support the medical necessity of the procedure. The 1199SEIU Benefit Funds maintain an appeals process for denied prior authorization requests. Review the denial letter for the specific reason and follow the steps outlined to file an appeal.
Where can I find related 1199SEIU forms?
FormsPal provides several related forms for 1199SEIU fund members and healthcare providers, including the 1199 Form, the 1199 Grievance Form, and the 1199 SEIU Form. Providers working with other insurance plans may also find the Aetna Prior Authorization Form and the Medical Management Authorization Form useful.