
With the help of the online PDF editor by FormsPal, you'll be able to fill in or alter statement claim premium reimbursement here. Our editor is continually evolving to deliver the very best user experience achievable, and that is thanks to our resolve for continuous development and listening closely to user feedback. It merely requires several simple steps:
Step 1: Access the PDF form in our tool by clicking on the "Get Form Button" at the top of this page.
Step 2: With this handy PDF editor, it is possible to accomplish more than merely fill in forms. Edit away and make your docs seem faultless with customized textual content put in, or modify the file's original input to excellence - all comes along with the capability to add any kind of pictures and sign the PDF off.
Pay close attention when filling out this document. Make sure all required fields are filled out properly.
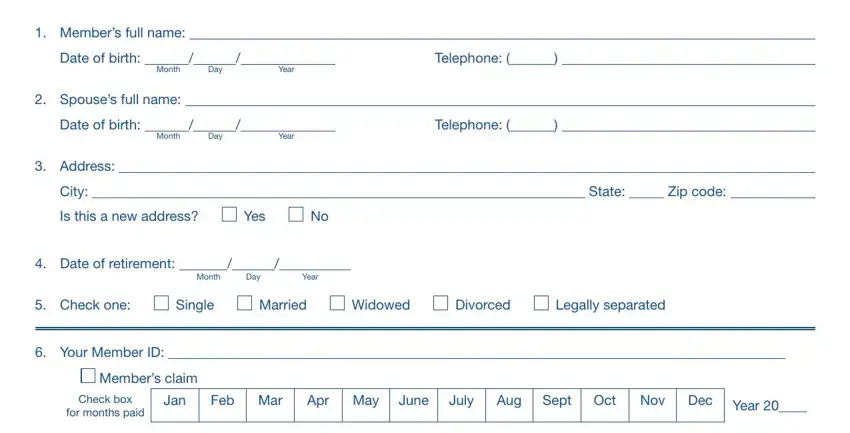
1. First of all, once filling out the statement claim premium reimbursement, start with the page containing next blank fields:
2. After performing the last section, go on to the subsequent step and complete all required particulars in these blank fields - Spouses claim, Check box, for months paid, Jan, Feb Mar, Apr May, June, July, Aug, Sept, Oct, Nov, Dec, Year , and Medicare Part B reimbursement will.
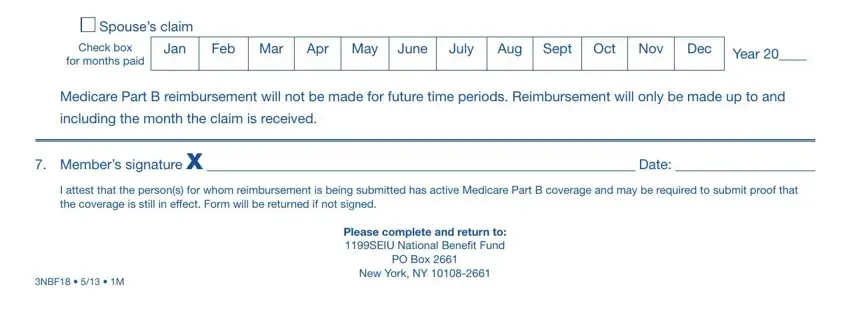
Be really careful while filling out for months paid and Year , as this is where a lot of people make errors.
Step 3: Right after taking another look at the completed blanks, click "Done" and you are all set! Download the statement claim premium reimbursement as soon as you register at FormsPal for a 7-day free trial. Conveniently view the pdf from your FormsPal account page, together with any modifications and changes conveniently preserved! We do not share or sell any details you use when filling out documents at FormsPal.