Filling out the ACD 1069 form is straightforward using our free online PDF editor. Follow these steps to complete and download your form:
Step 1: Open the form. Click the orange "Get Form Now" button at the top of this page. The ACD 1069 form opens directly in your browser, no software download required.
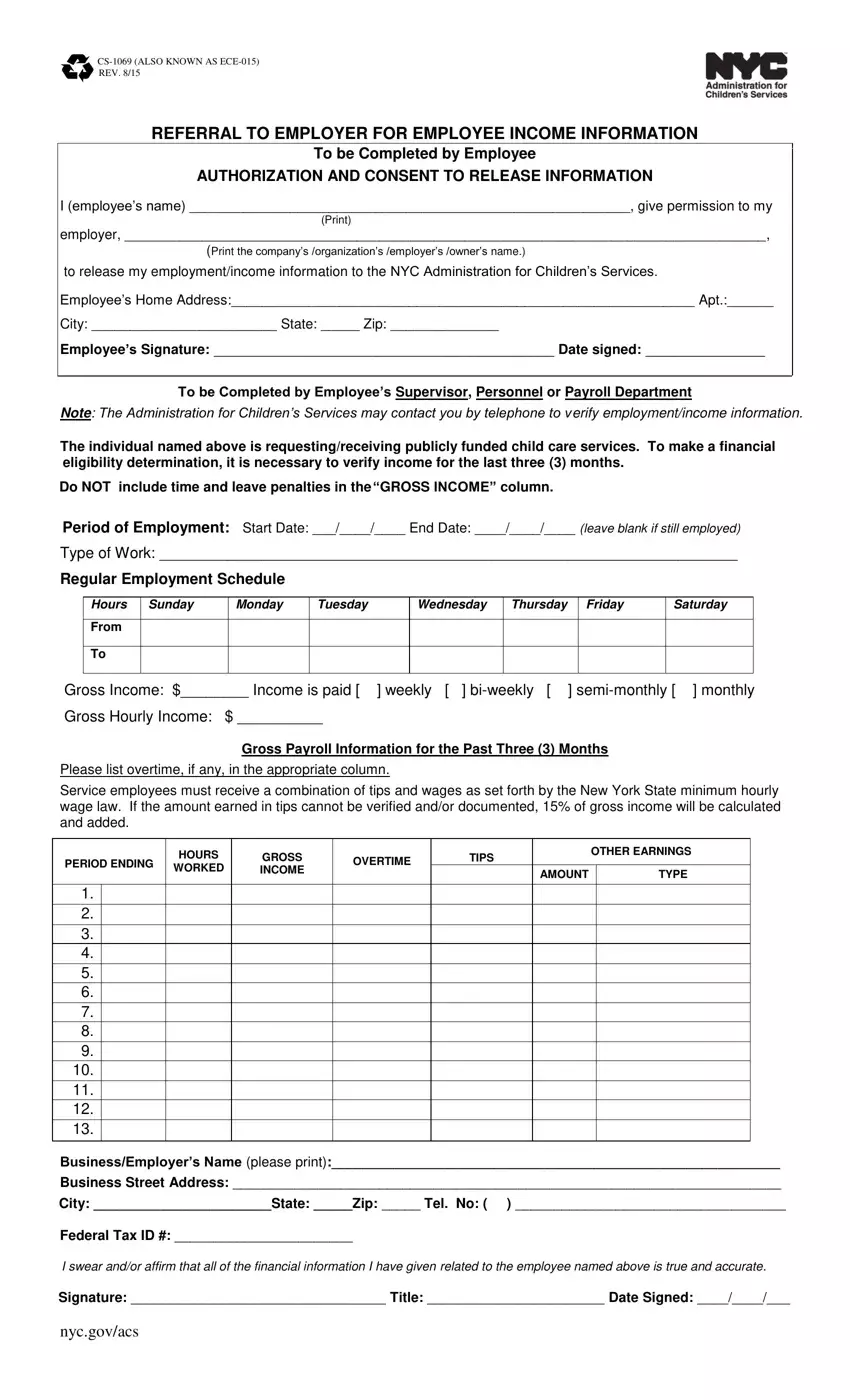
Step 2: Complete Part 1 (Income section). Enter the employee's name and employment type. Fill in the gross income for each week in the three-month period, listing amounts by day of the week. Report regular wages, overtime, and tips. Do not include time-and-leave penalties in the gross income total.
Step 3: Complete Part 2 (Employer certification). Enter the employer's business name, city, state, zip code, phone number, and Federal Tax ID. An authorized representative must sign and date the form, certifying that all reported income is accurate.
What information do you need to complete the ACD 1069 form? You will need the employee's full name, their regular work schedule and daily hours, gross earnings for each of the past three months broken down by week, the employer's legal business name and Federal Tax ID, and an authorized signature from a company representative.
Step 4: Save and submit. Click "Done" to download your completed ACD 1069 form as a PDF. You can save it to your device, print it, or send it by email. Submit the completed form to ACS as directed by the employee's caseworker.
For other NYC employment documents, see the CCIS Employment Verification form. Keep a copy of the completed form for your records. Your personal information is never stored or shared by our service.
