Our PDF editor allows you to fill in documents. You should not undertake much to modify par q acsm forms. Only keep up with the following actions.
Step 1: The first task should be to click on the orange "Get Form Now" button.
Step 2: At this point, you're on the file editing page. You may add content, edit current details, highlight certain words or phrases, put crosses or checks, insert images, sign the form, erase unneeded fields, etc.
The next few areas are what you are going to fill out to get the finished PDF document.
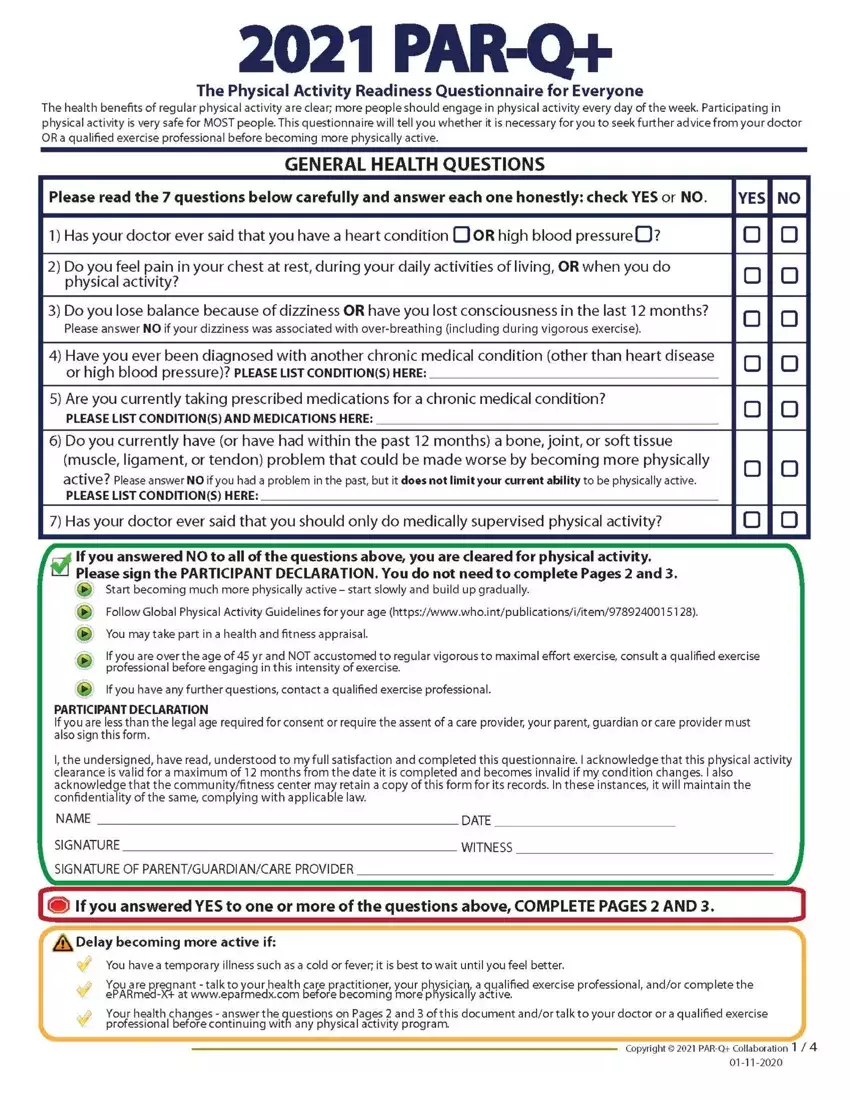
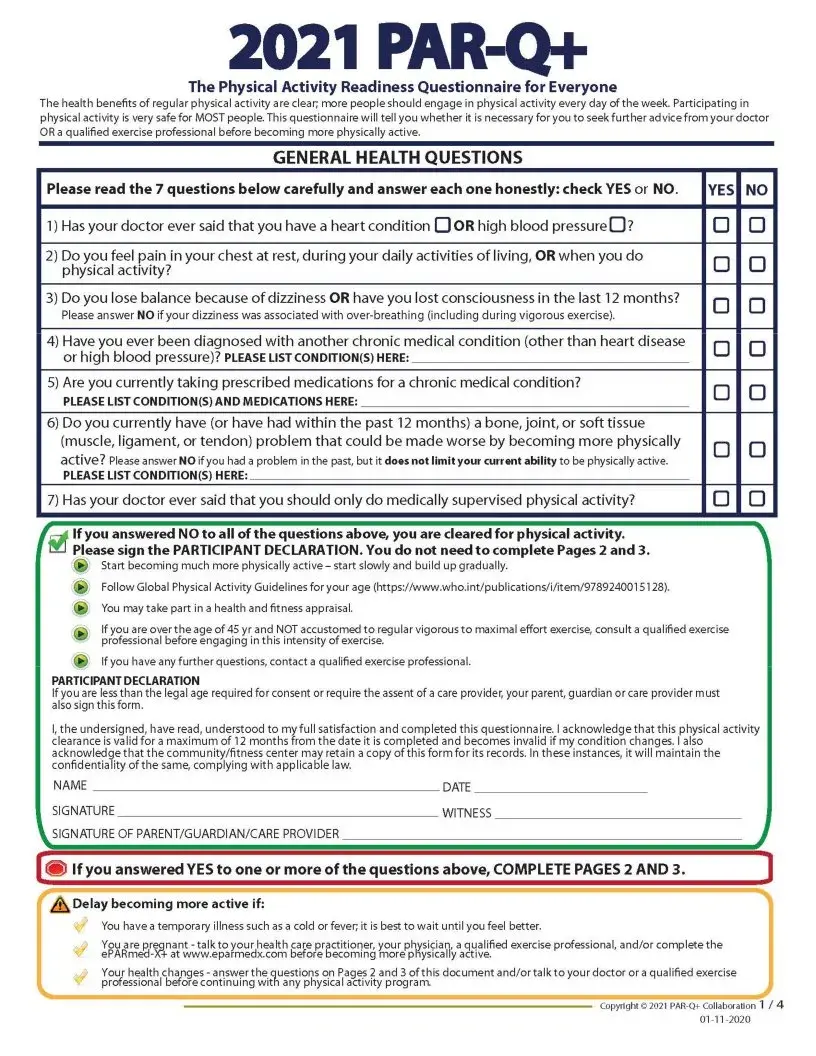
You should enter the appropriate data in the I clearance is valid for a maximum, NAME, SIGNATURE, SIGNATURE OF PARENTGUARDIANCARE, DATE, WITNESS, i If you answered YES to one or, Delay becoming more active if, You have a temporary illness such, You are pregnant talk to your, Your health changes answer the, and Copyright PARQ Collaboration area.
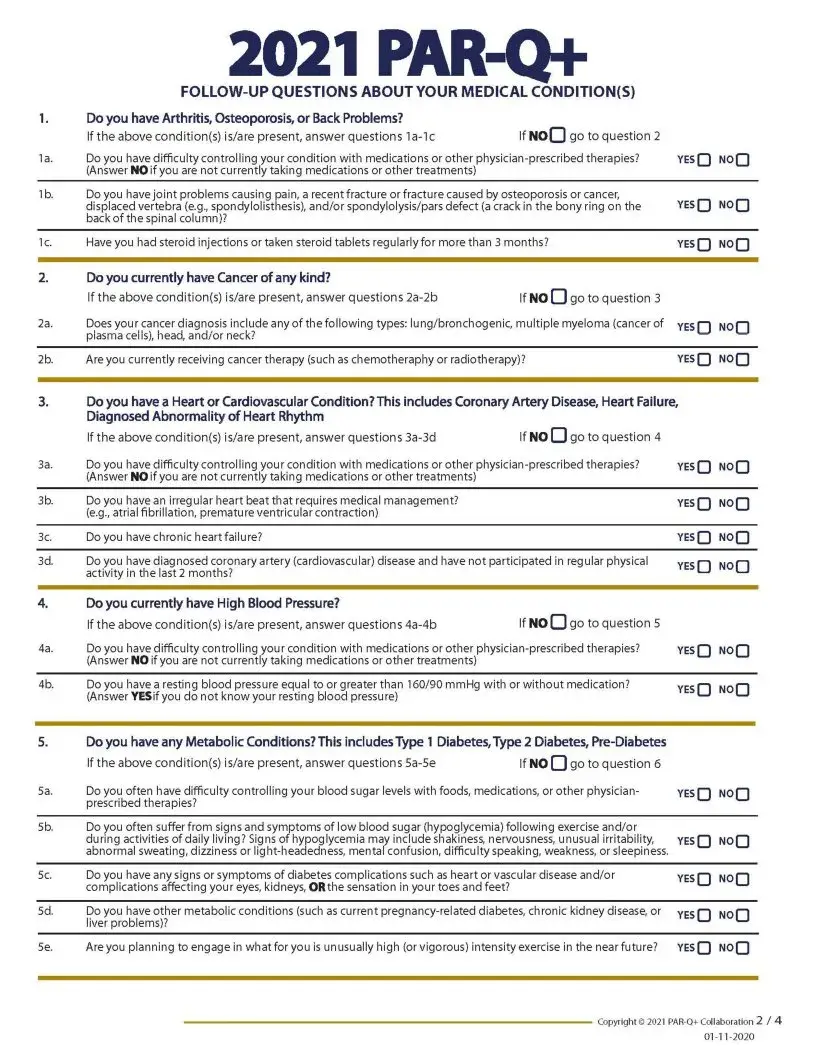
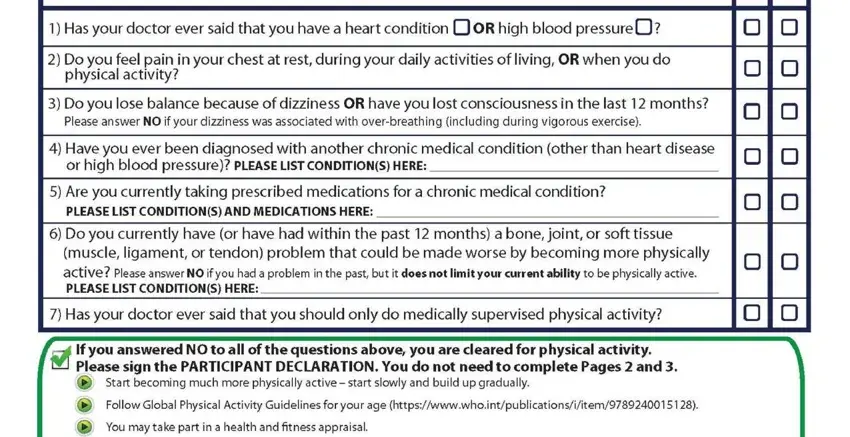
Indicate the vital particulars in Do you have Arthritis, If the above conditions isare, If noQ go to question, Do you have difficulty control, Do you have joint problems causing, Have you had steroid injections or, YESQ NOQ, Do you currently have Cancer of, If NO O go to question, a Does your cancer diagnosis, plasma cells head andor neck, b Are you currently receiving, YESQ NOQ, Do you have a Heart or, and go to question segment.
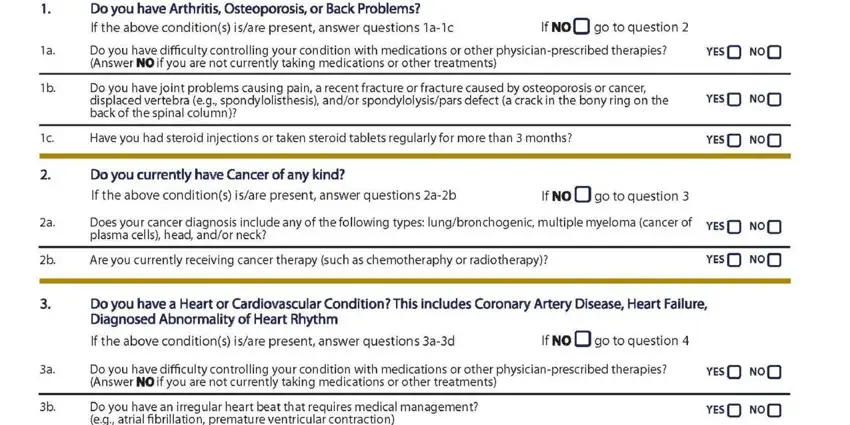
The Do you have an irregular heart, Do you have chronic heart failure, Do you have diagnosed coronary, Do you currently have High Blood, If NO O to question, yesQ NOQ, YESQ NOQ, Do you have difficulty controlling, yesQ NOQ, Do you have a resting blood, YESQ NOQ, Do you have any Metabolic, If the above conditions isare, If NO go to question, and Do you often have difficulty section will be the place to include the rights and responsibilities of each party.
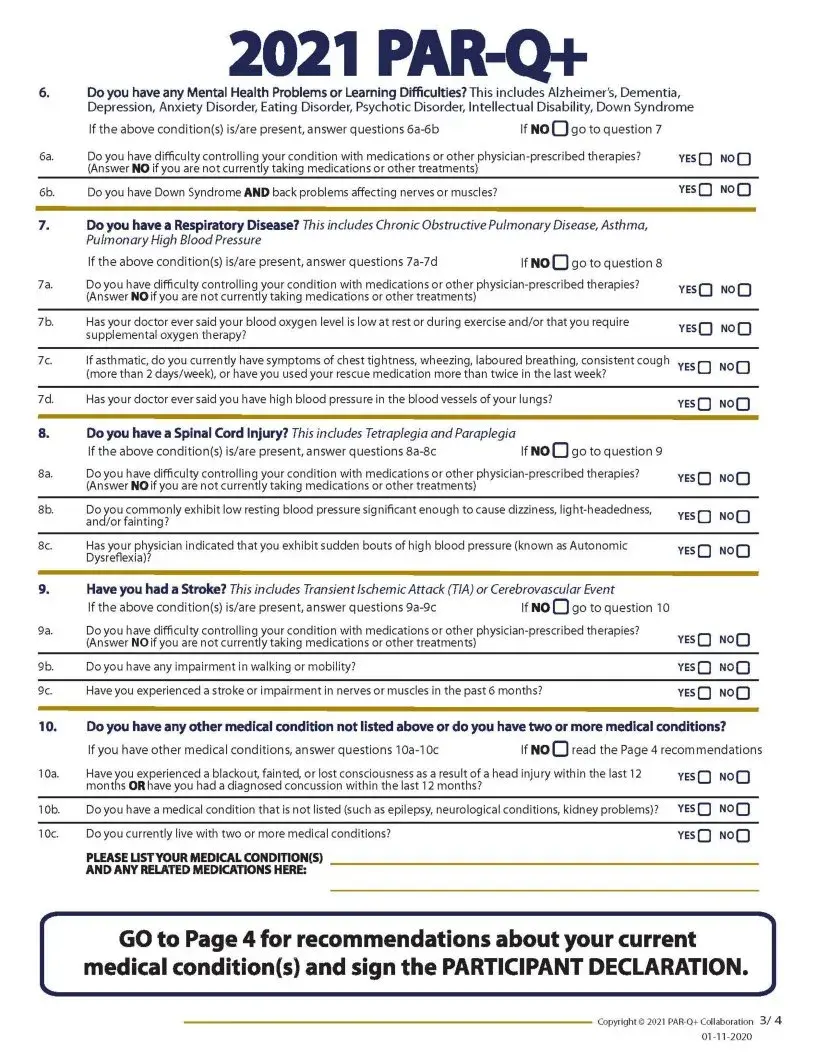
Complete the file by reviewing these areas: Are you planning to engage in what, YESQ NOQ, and Copyright PARQCollaboration.

Step 3: Choose the "Done" button. Now it's possible to export the PDF file to your device. Besides, it is possible to send it via electronic mail.
Step 4: Come up with as much as a few copies of the file to stay clear of all of the possible future concerns.
