


 Dental Claim Form
Dental Claim FormWe chose the top software engineers to make our PDF editor. Our software will help you create the ada dental claim form 2021 file with no trouble and won't take up too much of your time. This easy-to-follow instruction will help you get started.
Step 1: The following page includes an orange button saying "Get Form Now". Click it.
Step 2: When you have entered the editing page ada dental claim form 2021, you will be able to find each of the options available for your form at the upper menu.
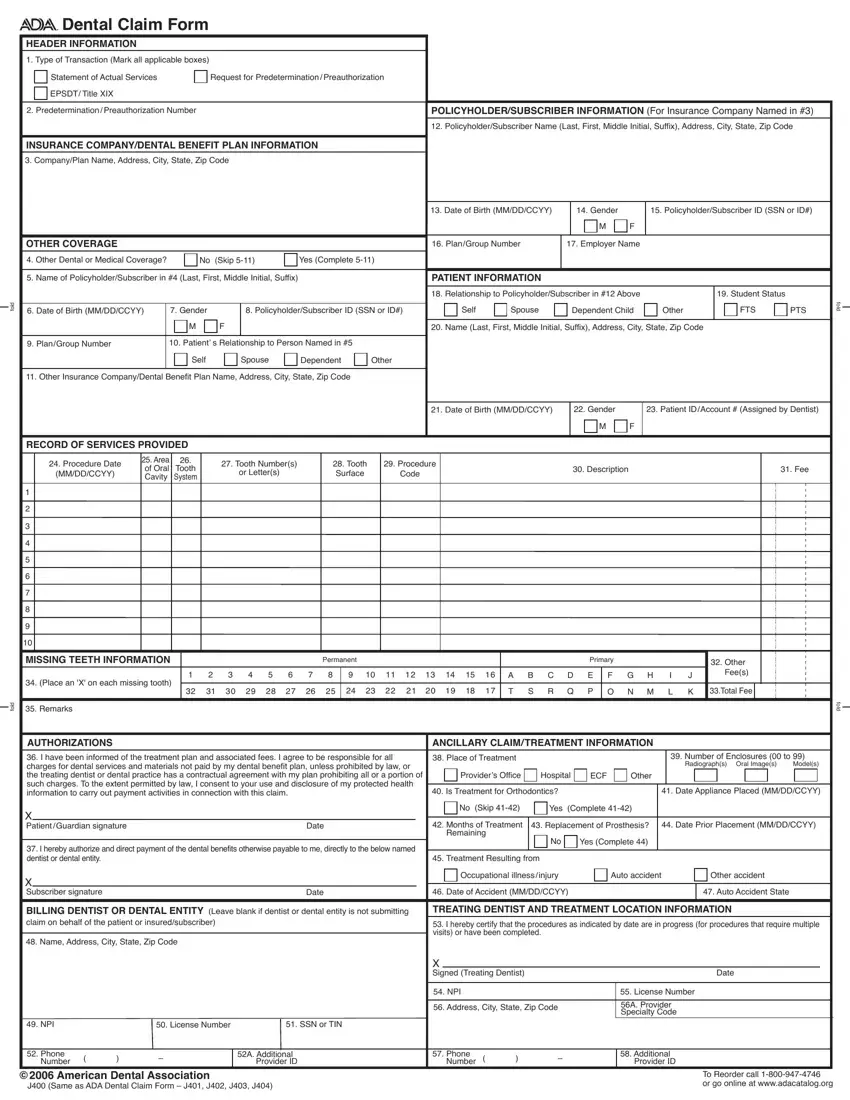
Feel free to type in the next information to fill out the ada dental claim form 2021 PDF:
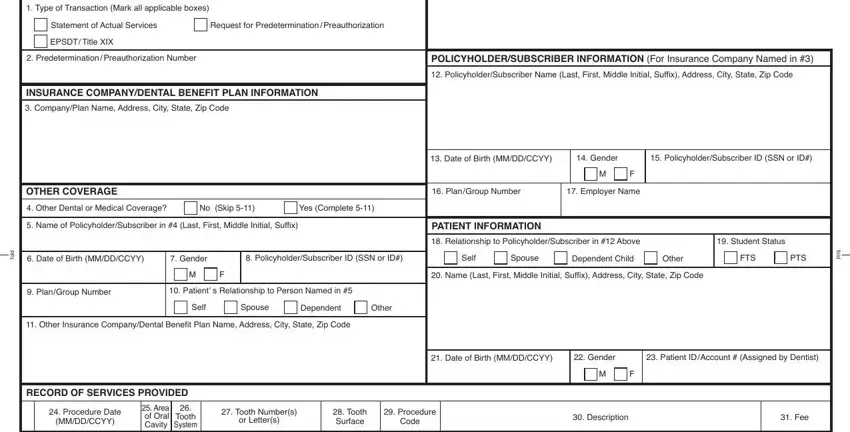
The system will demand you to fill out the MISSING TEETH INFORMATION, Permanent, Primary, Place an X on each missing tooth, A B C D E, F G H I, Other Fees, T S R Q P, O N M L K, Total Fee, d o f, Remarks, AUTHORIZATIONS, I have been informed of the, and ANCILLARY CLAIMTREATMENT field.
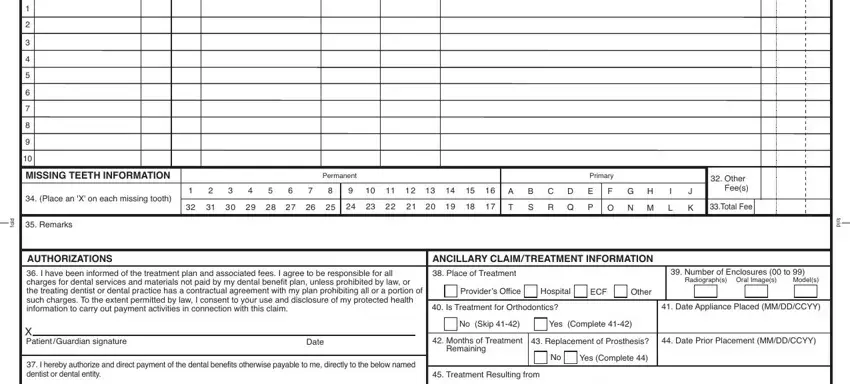
Record all information you are required within the space X Subscriber signature, Date, Date of Accident MMDDCCYY, Auto Accident State, Occupational illness injury, Auto accident, Other accident, BILLING DENTIST OR DENTAL ENTITY, TREATING DENTIST AND TREATMENT, I hereby certify that the, Name Address City State Zip Code, NPI, License Number, SSN or TIN, and Phone Number.
Step 3: If you are done, click the "Done" button to export the PDF document.
Step 4: To prevent yourself from different complications in the future, you should get a minimum of a few copies of your document.
