Completing the CSA Dental Claim Form is easy using the FormsPal PDF editor tools. Follow these steps to get the document ready and send it without delay.
Step 1: Click the orange "Get Form Here" button at the top of the page to open the PDF editor.
Step 2: The form editing page will load. You can enter text into the fields or update existing data as needed.
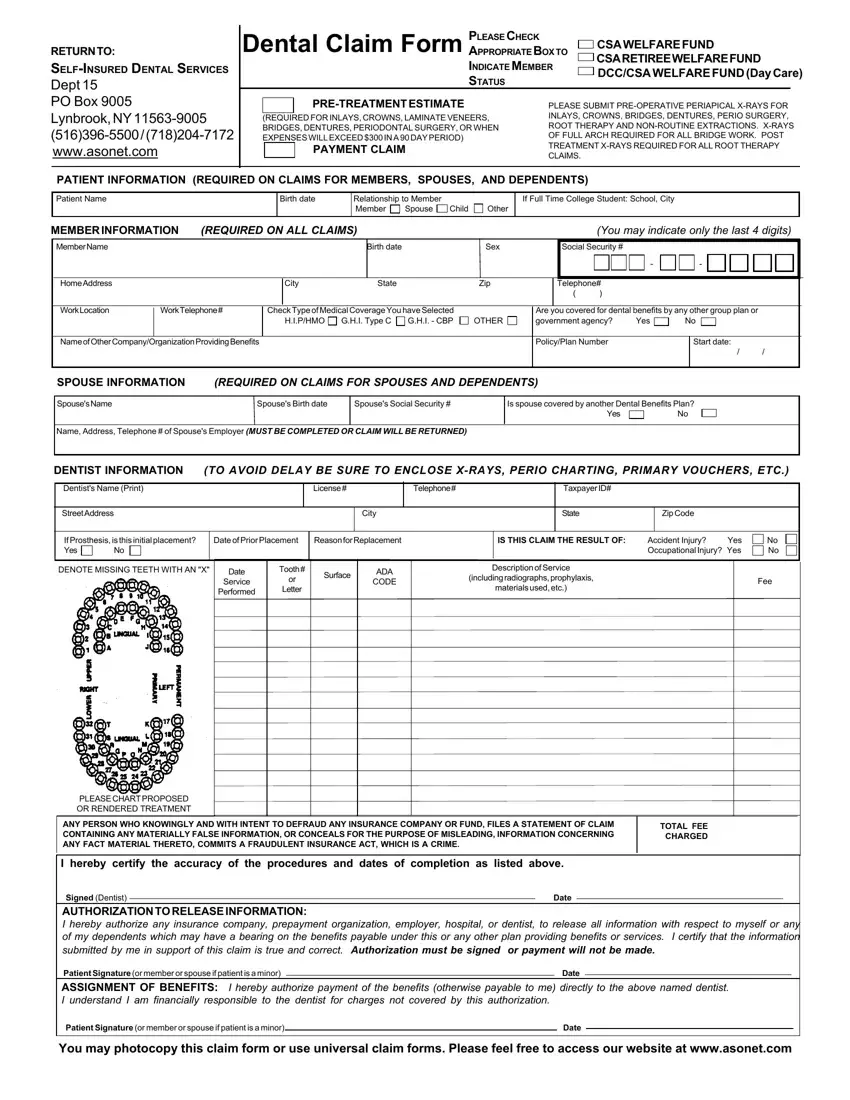
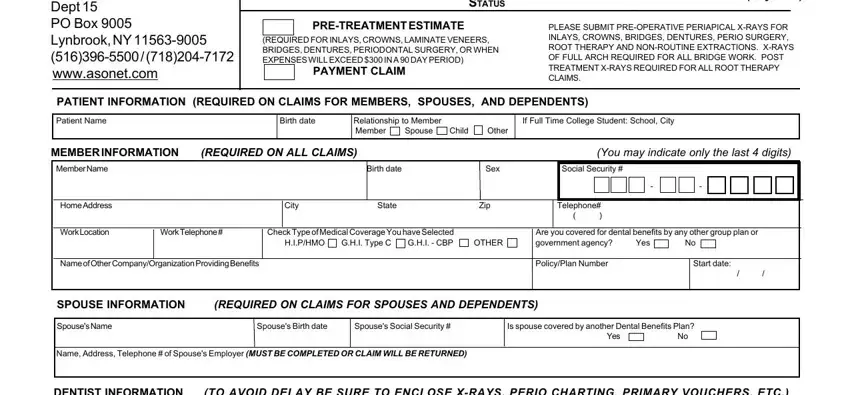
Please enter all required information to complete the CSA dental claim form:
Fill out the DENTIST INFORMATION section, including the Dentist Name (Print), License number, Telephone, Taxpayer ID, Street Address, City, State, and Zip Code. In the appropriate box, indicate whether the prosthesis is initial, enter the Date of Prior Placement, and provide the Reason for Replacement. Mark the field indicating whether this claim is the result of an accident or injury.
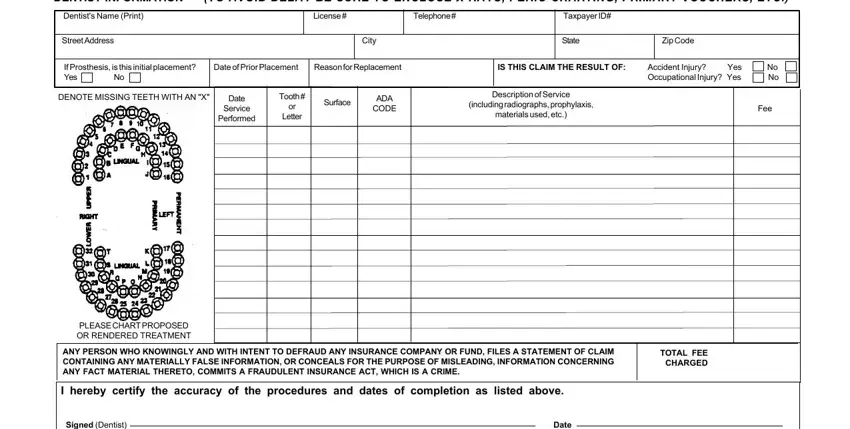
In the signature section, complete the Dentist Authorization to Assign Benefits. The patient or member signs and dates the form. Please review all data carefully before submitting. You may photocopy this claim form to keep a copy for your personal records.

Step 3: Click "Done" when you have finished entering all information. You can then download, print, or send the completed PDF.
Step 4: Keep at least two copies of the completed form before sending it to the administrative office. This helps you manage your records and provides documentation in case of any follow-up questions.
Related Dental Claim Forms
If you need to complete other dental benefit claim forms, these resources may also be useful:
