We built this PDF editor to make the process as simple as possible. Follow the steps below to fill out the CSA Damage Form quickly and accurately.
Step 1: Open the Form
Click the orange "Get Form Now" button at the top of this page. The form opens directly in the editor. No downloads are required.
Step 2: Enter Your Personal and Property Details
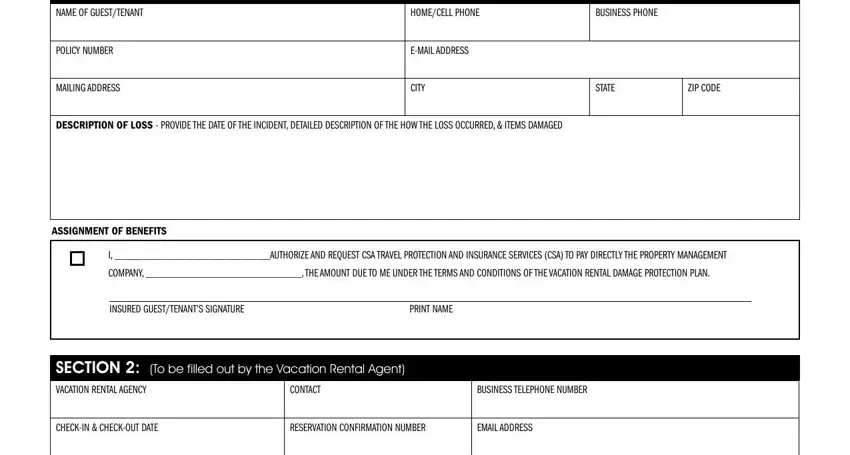
Fill in your name, home phone, cell phone, business phone, policy number, and mailing address. Add your email, city, state, and zip code. Include a description of the loss and enter any assignment of benefits details. Sign and print your name in the guest signature area.
Complete each field in the guest section. Use your coverage documents if you need help locating your policy number.
Step 3: Document the Property Damage
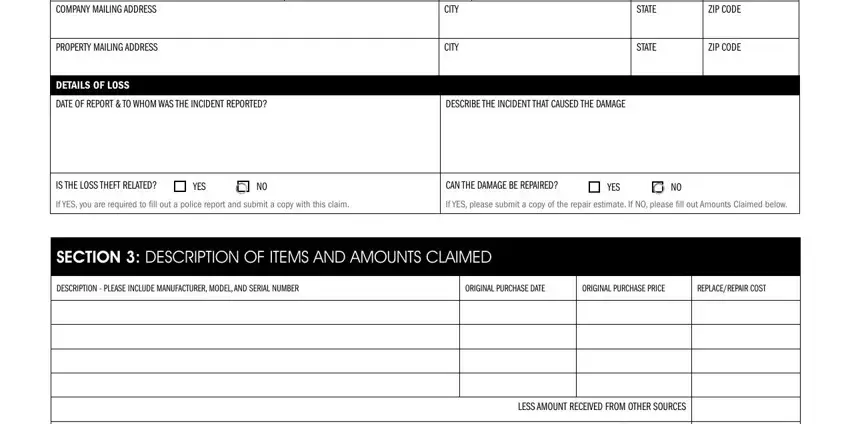
Enter the company mailing address and property mailing address. Describe the details of the loss clearly. Include the city, state, and zip code for the property. Note the date of the report and who was notified. Describe the incident that caused the damage. State whether the loss is theft-related and whether the damage can be repaired.
Step 4: Review Disclosures and Sign
Read the fraud warnings and disclosures section. Check the acknowledgment box. Both the guest and the vacation rental agent must sign and print their names. Add the date of each signature. If the claim involves theft, attach a copy of the police report. You may submit the completed form by email or mail to CSA.
When you click the Done button, your form is ready to download or send. Keep two or three copies for your records.
For other damage-related documents, see the vehicle accident or damage report and the statement of damages form.
