We've used the endeavours of the best programmers to build the PDF editor you intend to take advantage of. Our software will assist you to fill in the cvs otc catalog 2021 aetna document effortlessly and don’t waste time. Everything you should undertake is follow these particular simple rules.
Step 1: Choose the "Get Form Here" button.
Step 2: So, you are on the form editing page. You may add text, edit existing details, highlight specific words or phrases, put crosses or checks, insert images, sign the file, erase unnecessary fields, etc.
Feel free to type in the following information to complete the cvs otc catalog 2021 aetna PDF:
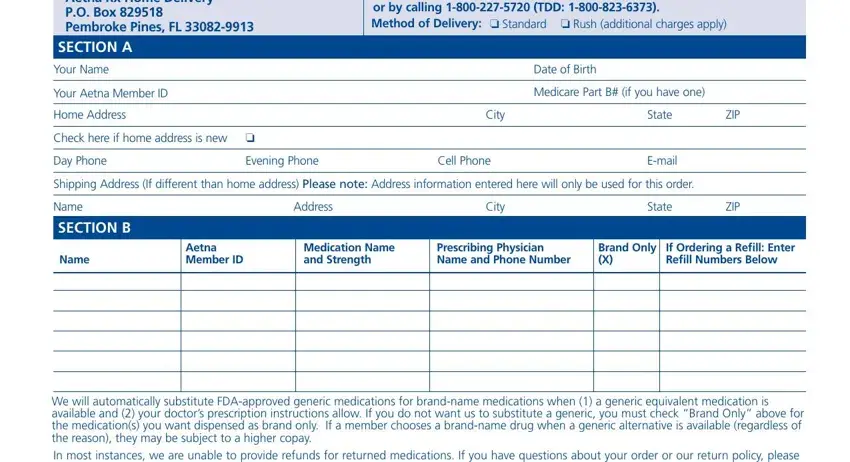
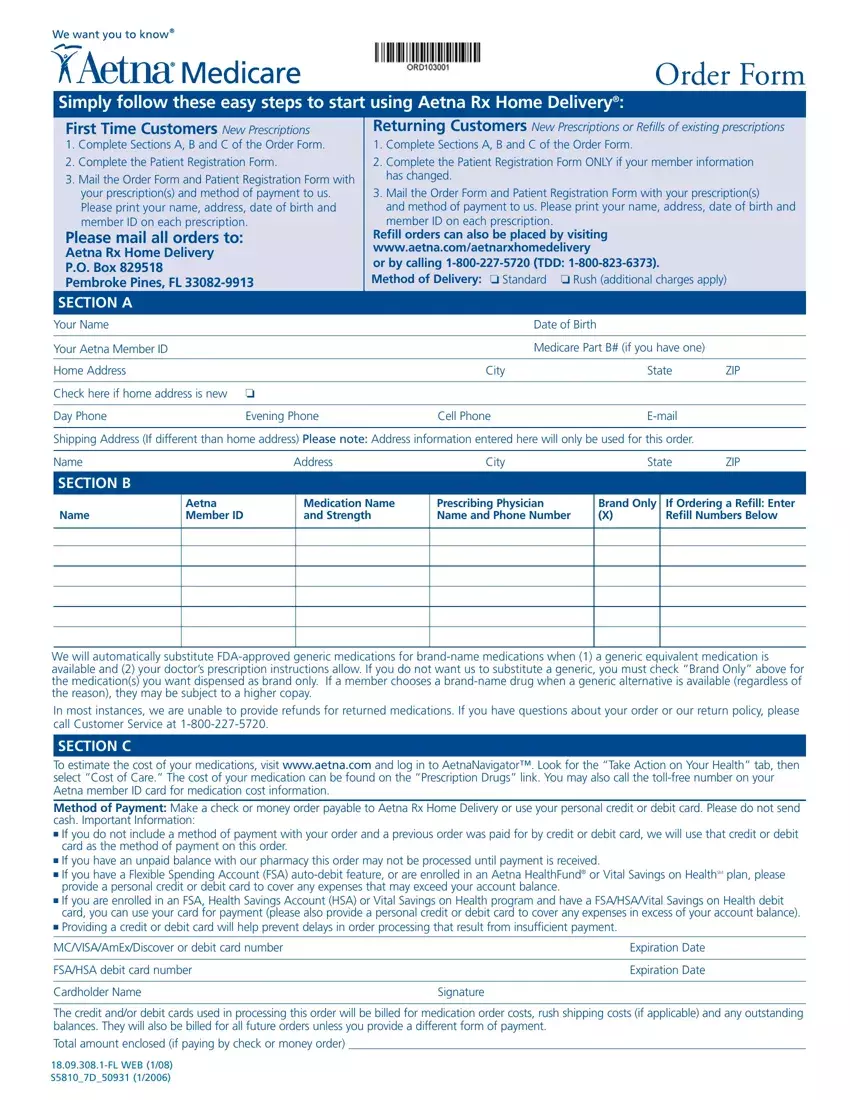
Feel free to complete the SECTION C To estimate the cost of, card as the method of payment on, If you have an unpaid balance, provide a personal credit or debit, If you are enrolled in an FSA, card you can use your card for, Providing a credit or debit card, MCVISAAmExDiscover or debit card, FSAHSA debit card number, Cardholder Name, Signature, Expiration Date, Expiration Date, The credit andor debit cards used, and FL WEB SD space with the essential data.
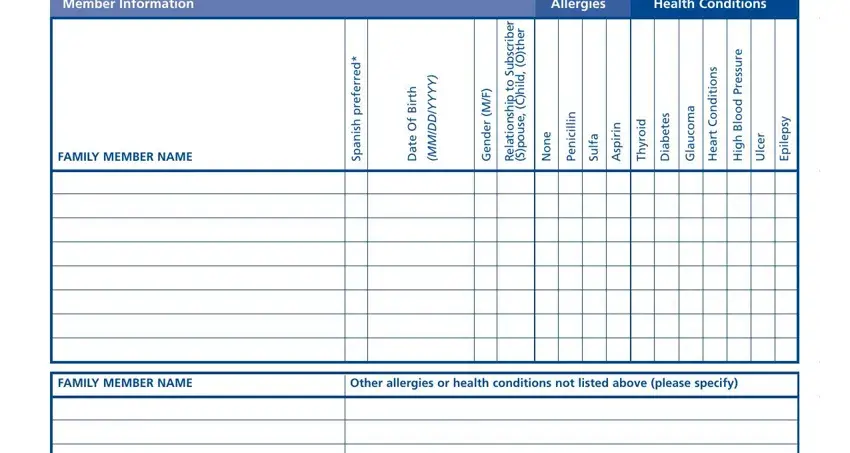
Write down the key data in Member Information, Allergies, Health Conditions, d e r r e f e r p h s i n a p S, h t r i B f O e t a D, FAMILY MEMBER NAME, Y Y Y Y D D M M, F M, r e d n e G, r e b i r c s b u S o t p h s n o, r e h t O, l i, h C, e s u o p S, and i l l i c i n e P part.
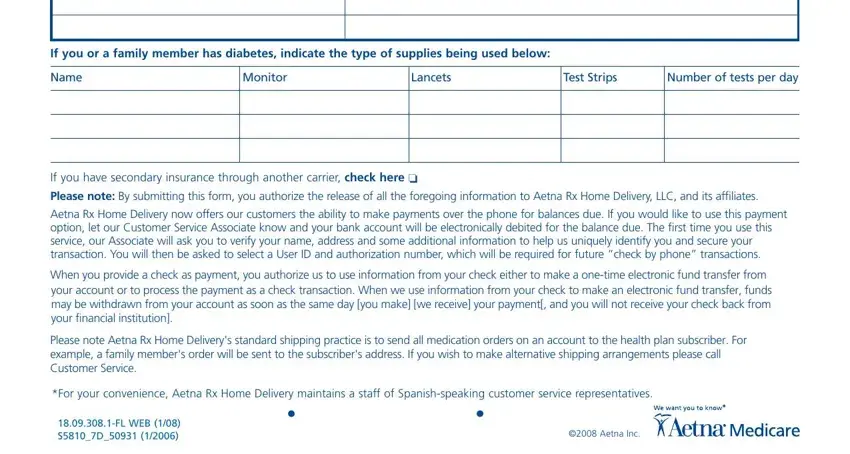
When it comes to part If you or a family member has, Name, Monitor, Lancets, Test Strips, Number of tests per day, If you have secondary insurance, Aetna Rx Home Delivery now offers, When you provide a check as, Please note Aetna Rx Home, For your convenience Aetna Rx Home, FL WEB SD, and Aetna Inc, state the rights and obligations.
Step 3: Click the Done button to be sure that your finalized file can be exported to any type of gadget you prefer or forwarded to an email you specify.
Step 4: Prepare a duplicate of each separate form. It should save you time and permit you to avoid troubles later on. By the way, your details is not shared or viewed by us.
