
Follow these steps to fill out and submit the allergenic extract claim form correctly and avoid delays in reimbursement.
Step 1: Gather your documents. Before you begin, collect your health plan ID card, an itemized bill from your pharmacist or physician, and the exact dates of service for the allergenic extract you received.
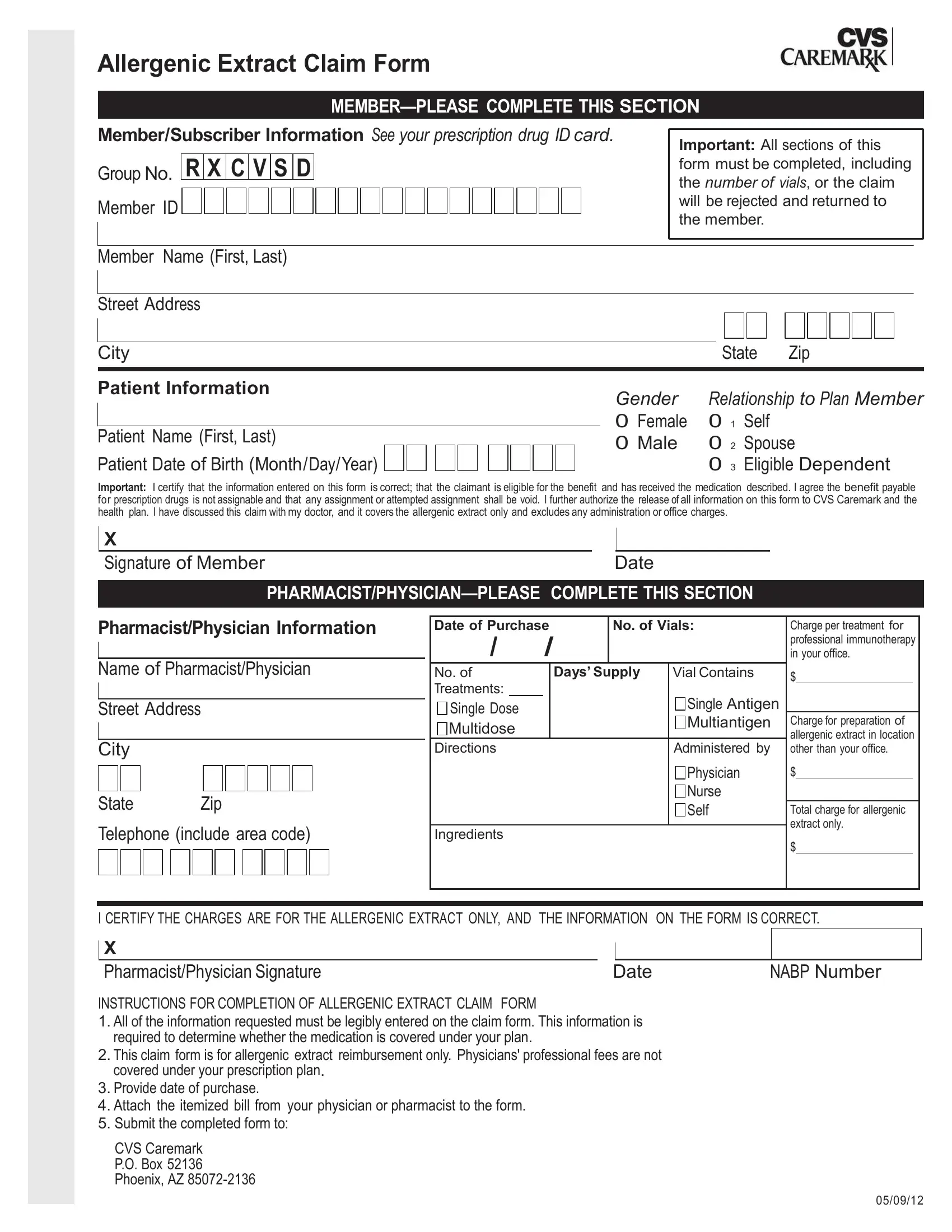
Step 2: Complete the member section. Enter your full name, address, and subscriber ID number. Include the patient's information if you are submitting on behalf of a dependent. Confirm that the allergenic extract was received and that all charges listed are exclusively for the extract. Do not include fees for office visits or injection administration.
Step 3: Have your provider complete their section. Ask your dispensing pharmacist or physician to fill in the number of vials dispensed, the cost per vial, and the total charge. Their signature is required to certify that only allergenic extract charges are included.
Step 4: Attach the itemized bill. Clip the itemized bill from your provider to the completed form. The bill must show the date of service and the exact charge for the allergenic extract.
Step 5: Mail your submission. Send the completed form and itemized bill to the address printed on the form or provided by your plan. Keep a copy of everything for your records. Processing typically takes up to 30 days. For other healthcare expense claims, see the medical claim form or the Healthscope medical claim form.