
Completing the SCAT application form online is straightforward with our PDF editor. Anyone can fill in the scat application form here and access features including custom text, signatures, and editing tools. It takes just a few steps:
Step 1: Click on the orange “Get Form” button above. It will open our editor so you can begin completing your form.
Step 2: As you access the editor, the document will be ready to complete. You can fill out fields, add custom text, edit existing content, insert graphics, place your signature, and more.
When completing the scat application form, here is what to do for each section:
1. First, when completing the scat application form, start with the section containing these fields:
2. Fill out all of these fields: STREET ADDRESS, APTBLDG, CITY, COUNTY, ZIP CODE, Do you require information, Mark all that you need, Braille, Large Print, Audio Tape, Other, PLEASE GIVE US THE NAME AND, LAST NAME, FIRST NAME, and HOME PHONE NUMBER with their corresponding information. Double-check all entries before continuing.
3. The next portion covers: Please indicate below if you use, Cane, Crutches, Long white cane for the visually impaired, Manual wheelchair, Powered wheelchair, Powered scooter/cart, Service/guide animal, Respirator/oxygen tank, Walker, Leg braces, Other, I don't require any assistive devices, and PART QUESTIONS ABOUT USING FIXED ROUTE. Complete these fields carefully.
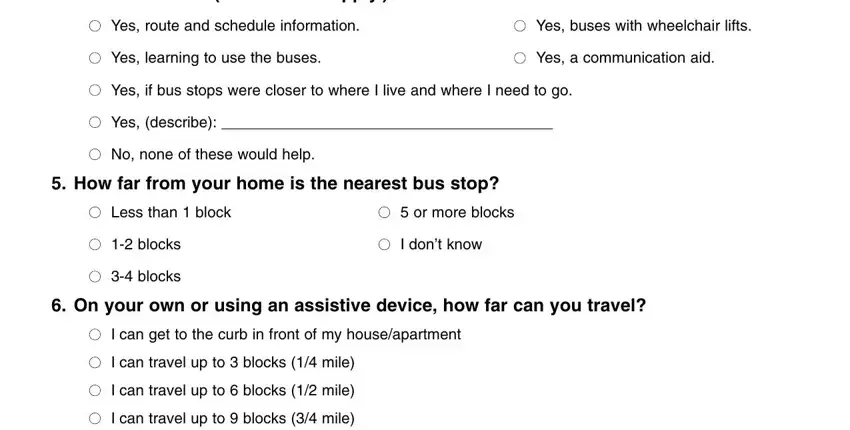
4. Completing the section about riding buses is important. Mark all that apply: Yes to route and schedule information, Yes to buses with wheelchair lifts, Yes to learning to use the buses, Yes to a communication aid, Yes if bus stops were closer to your location, No none of these would help, and how far from your home is the nearest bus stop. Also indicate whether you can reach a bus stop on your own or with an assistive device.
5. Complete the final section with all remaining required fields.

Be careful when completing the final fields to avoid errors.
Step 3: Verify all information is correct, then click "Done" to finish. Sign up to save and access the scat application form anytime. FormsPal.com keeps your information private and secure.
Other disability and accessibility forms available on FormsPal: disability parking certificate, disability questionnaire form, and disability claim form.