
You can fill out this religious beliefs exemption form easily using our PDFinity® editor. Our expert team works continuously to improve the tool and make it simple and reliable for every user. Follow these steps to complete and save your form accurately.
Step 1: Open the tool by clicking the "Get Form Button" at the top of this page.
Step 2: Use the PDF editor to fill in required fields, add text, adjust existing content, upload images, and add your electronic signature.
For you to fill out this PDF document, be sure to type in the information you need in each blank field:
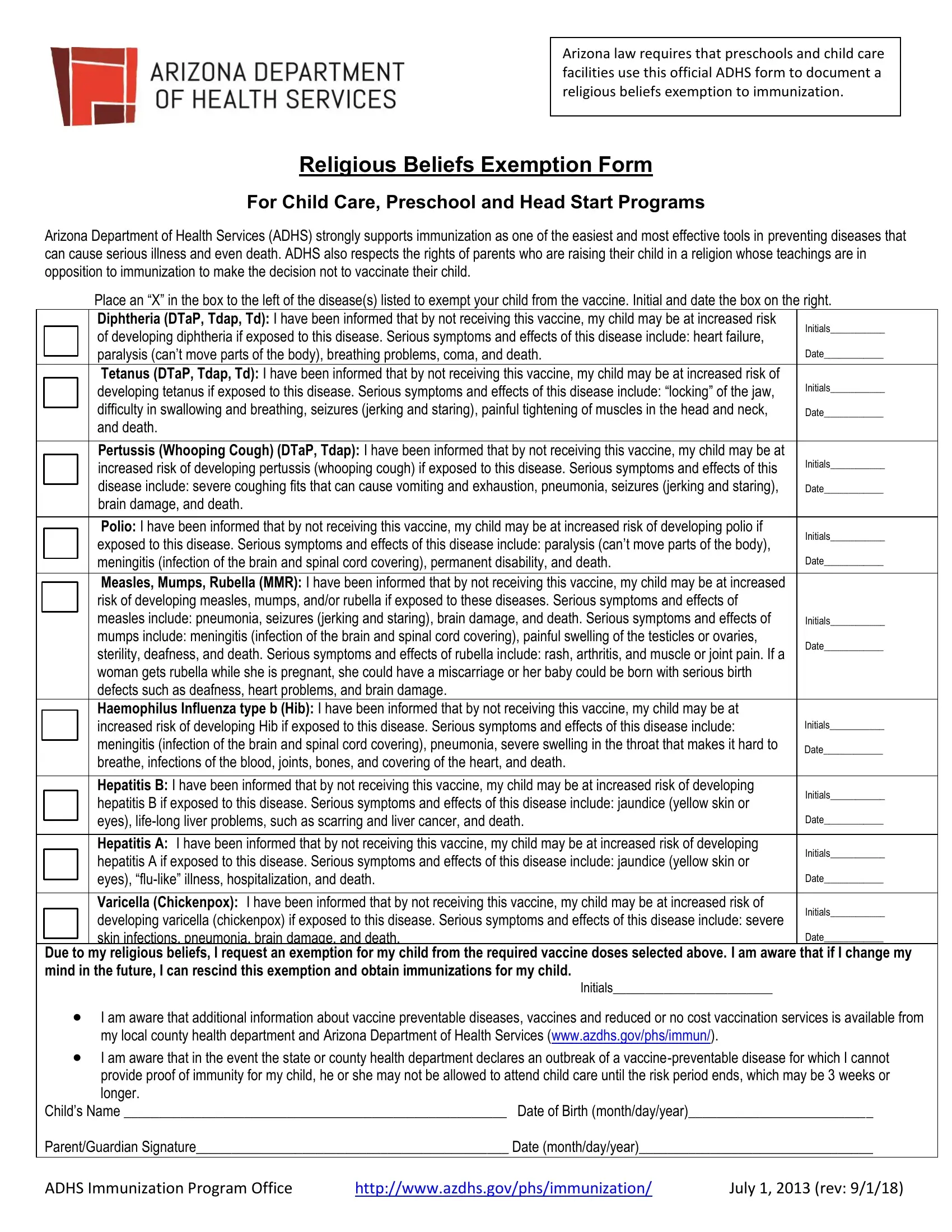
1. Fill out the first section of the religious beliefs exemption carefully, paying attention to these fields:
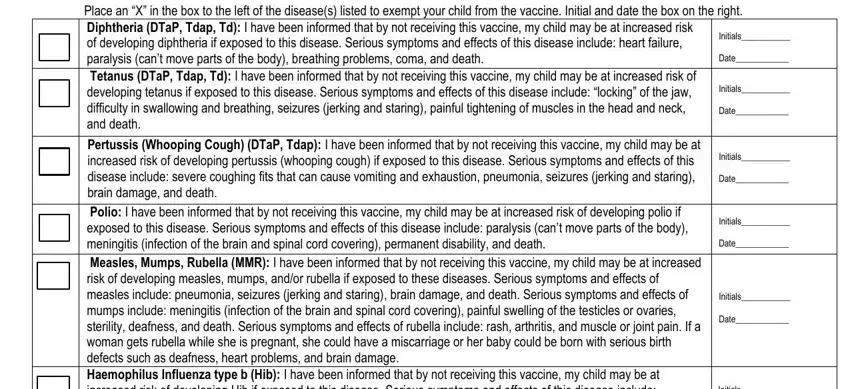
2. After the first section, proceed to enter information in these fields: Polio I have been informed that by, Initials Date, Hepatitis B I have been informed, Initials Date Initials Date, Due to my religious beliefs I, I am aware that additional, and Childs Name Date of Birth.
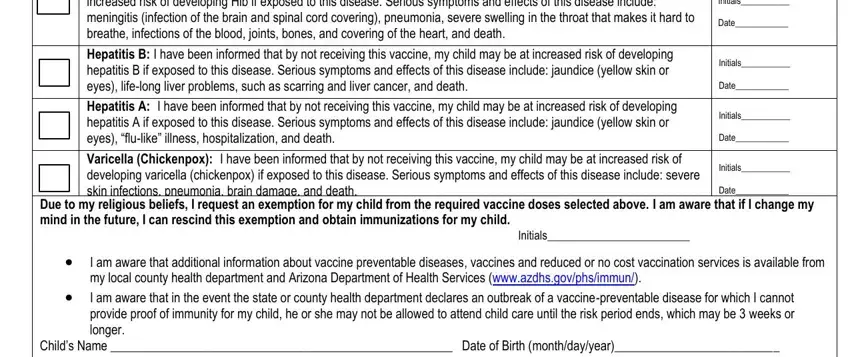
Take extra care when filling out the "I am aware that additional" and "Initials Date Initials Date" fields. Errors in these sections are the most common mistakes people make when completing the form.
3. Completing "Childs Name Date of Birth" and the ADHS Immunization Program Office fields is required before you can finalize the form. Do not leave these blank.

Step 3: Before finishing, review every field to confirm the information is correct. When you are satisfied, click "Done." Sign up for a FormsPal account to save the form and return to edit it at any time. We never sell or share the information you enter on FormsPal.
Where to Submit the Completed Arizona Exemption Form
After completing the form, submit it directly to the child care facility, preschool, or Head Start program where your child will be enrolled. The facility is required to keep this document on file as part of the child's enrollment records. Do not mail the form to ADHS directly. The child's school or child care center is the correct point of submission.
If you have questions about the submission process, contact your child's enrollment coordinator at the facility. You can also reach the ADHS Immunization Program Office, whose contact information is printed on the official form.
When Is the Arizona Religious Beliefs Form Needed?
The form must be submitted at or before the time of enrollment in a licensed Arizona preschool, child care center, or Head Start program. It is part of the required health documentation package for all new students. If your child changes facilities, the new school may ask for a current copy of the exemption form rather than accepting a transfer of the record from the previous location.
If your views change and you decide to vaccinate your child, notify the facility so that the exemption status can be updated. The facility will need to record the updated vaccination information and remove the exemption filing from the child's active record.
Other Vaccine Exemption and Health Forms
If you need a vaccine exemption form for a different state, the following forms are available on FormsPal:
For other health documentation that may be required for Arizona child care enrollment, you may also need the Child and Adolescent Health Form.