There is nothing troublesome in relation to completing the uhc personal representative form after you open our PDF tool. By taking these basic steps, you can receive the fully filled out document in the shortest time frame you can.
Step 1: Seek out the button "Get Form Here" and then click it.
Step 2: You're now on the document editing page. You can edit, add content, highlight certain words or phrases, place crosses or checks, and include images.
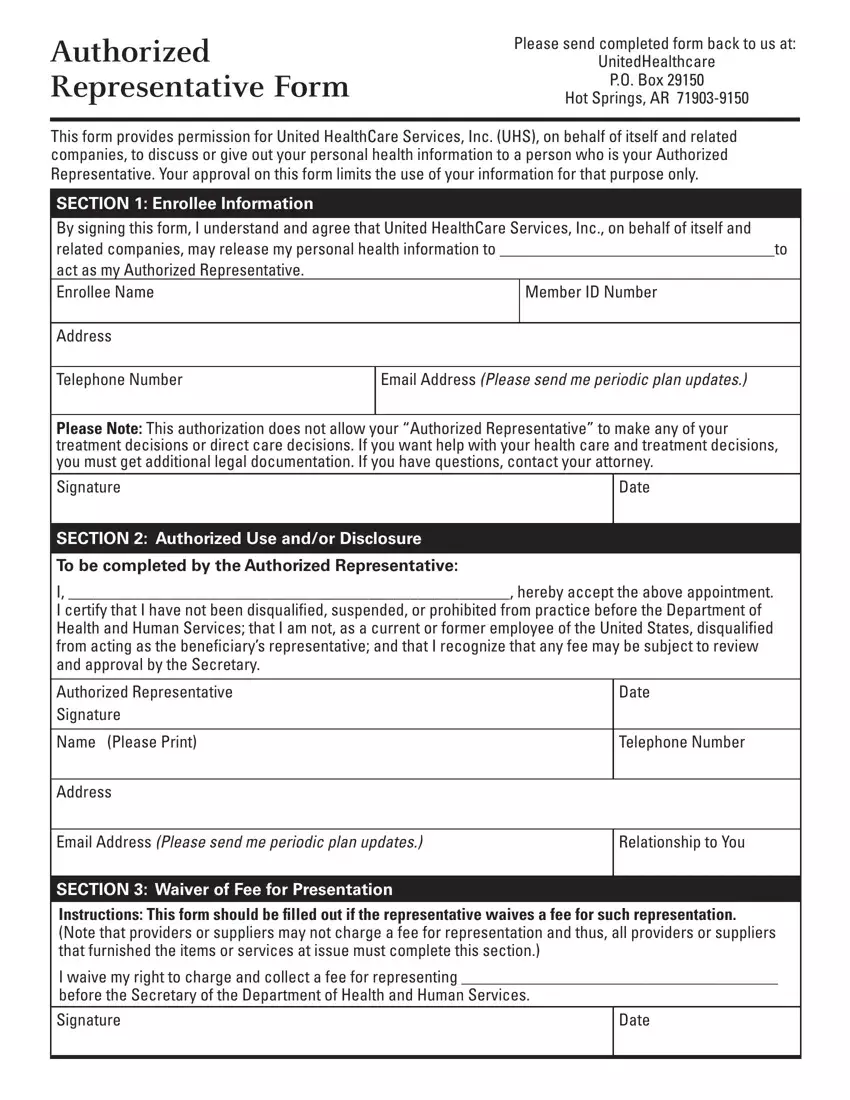
If you want to prepare the template, type in the data the application will request you to for each of the appropriate sections:
Make sure you provide the crucial details in the Authorized Representative Signature, Name Please Print, Address, Date, Telephone Number, Email Address Please send me, Relationship to You, SECTION Waiver of Fee for, I waive my right to charge and, and Date field.
You will need to insert particular particulars inside the space Signature, Date, SECTION Expiration and Revocation, I understand that I have the right, and CHARGING OF FEES FOR REPRESENTING.
Step 3: When you have clicked the Done button, your document should be ready for upload to any kind of electronic device or email you identify.
Step 4: Get as much as several copies of your form to stay away from any sort of future concerns.
