Completing the UHC personal representative form is straightforward when you use our online PDF editor. Follow the steps below to fill out your document quickly and accurately.
Step 1: Click the "Get Form Here" button on this page to open the document in the PDF editor.
Step 2: You are now on the document editing page. You can add text, highlight fields, place checkmarks, and make any necessary adjustments to the form.
If you want to prepare the template, type in the data the application will request for each section:
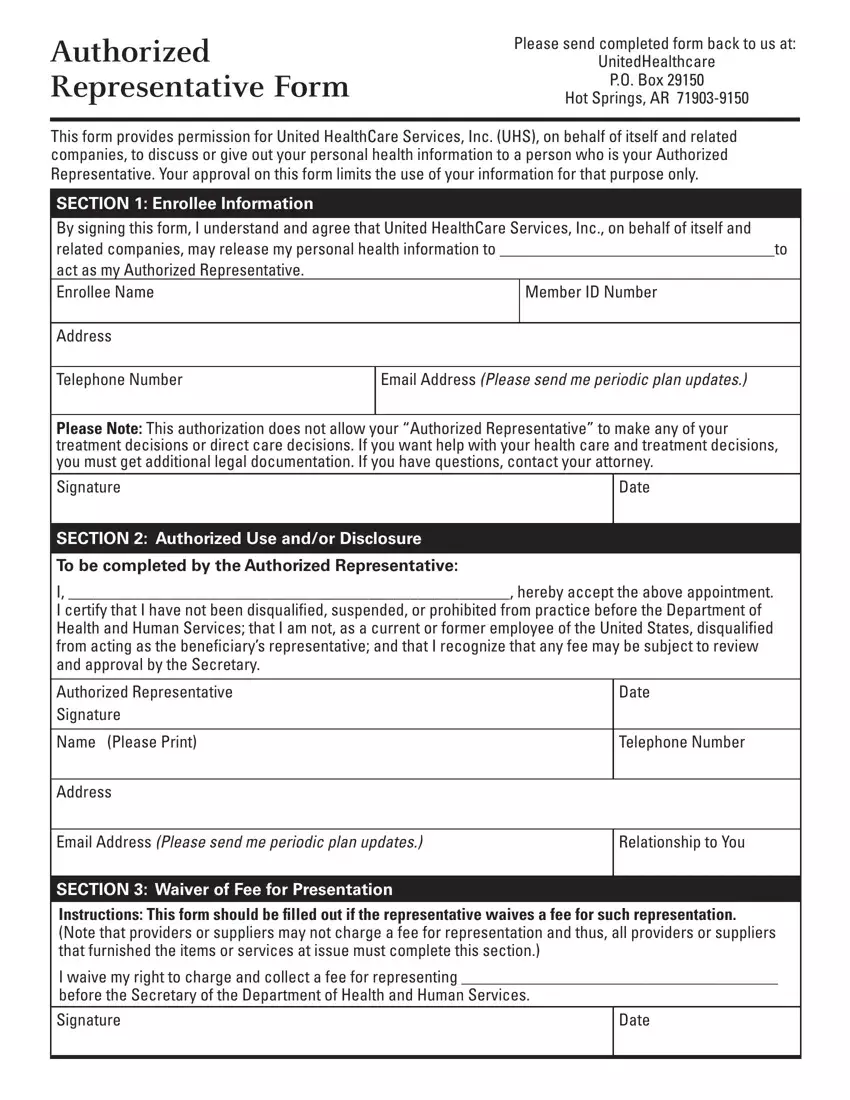
Complete the following required fields: Authorized Representative Signature, Name (Please Print), Address, Date, Telephone Number, Email Address, Relationship to You, Section for Waiver of Fee, and the I waive my right to charge field.
You will also need to complete the Signature field, Date, the Expiration and Revocation section, the statement beginning with "I understand that I have the right," and the Charging of Fees for Representing section.
Step 3: Click the Done button when you have finished. Your completed document will be ready to save, print, or send by email.
Step 4: Save or print multiple copies of the form for your records. It is a good practice to keep one copy with your insurance documents and provide one to your authorized representative.
Frequently Asked Questions
What is the difference between an authorized representative and a power of attorney?
An authorized representative form grants a named individual permission to access and share your health information with your insurance plan. A power of attorney is a broader legal instrument that may grant authority over financial decisions, medical choices, or other legal matters. For healthcare information purposes related to UnitedHealthcare, the authorized representative form is the correct document to complete and submit.
Can a parent or guardian be listed as an authorized representative?
Yes. Parents, legal guardians, attorneys, and other trusted individuals can all be named as an authorized representative. The form includes a field to specify the relationship between the enrollee and the representative, which helps clarify the nature and scope of the authorization.
How long does the authorization remain valid?
The authorization remains in effect until the enrollee provides written notice to revoke it or until any expiration date specified on the form has passed. The enrollee can cancel the authorization at any time by submitting a written request to United HealthCare Services, Inc. It is important to review the revocation terms in the form before signing.
What happens if I need to update or change my authorized representative?
To change your designated representative, you will need to revoke the existing authorization in writing and then submit a new completed form naming the updated individual. The website for UnitedHealthcare provides guidance on where to submit these documents.
Are there related forms I may also need?
Depending on your situation, you may benefit from reviewing these related documents available on FormsPal. The General Power of Attorney Form is useful when broader legal representation is required across multiple areas. The Representative Payee Report applies to social security benefit cases where a payee manages funds on behalf of a beneficiary. For healthcare planning purposes, the Advance Healthcare Directive outlines your medical wishes and designates decision-makers. If privacy and health data release are your primary concerns, the HIPAA Authorization Form is a closely related document that governs the release of medical records.
