
This PDF editor was developed to be as easy as possible. When you stick to the following actions, the procedure for preparing the 800 869 7093 file will be convenient.
Step 1: First of all, select the orange "Get form now" button.
Step 2: Now you are on the document editing page. You can edit, add content, highlight particular words or phrases, place crosses or checks, and put images.
If you want to fill in the template, type in the details the application will request you to for each of the appropriate areas:
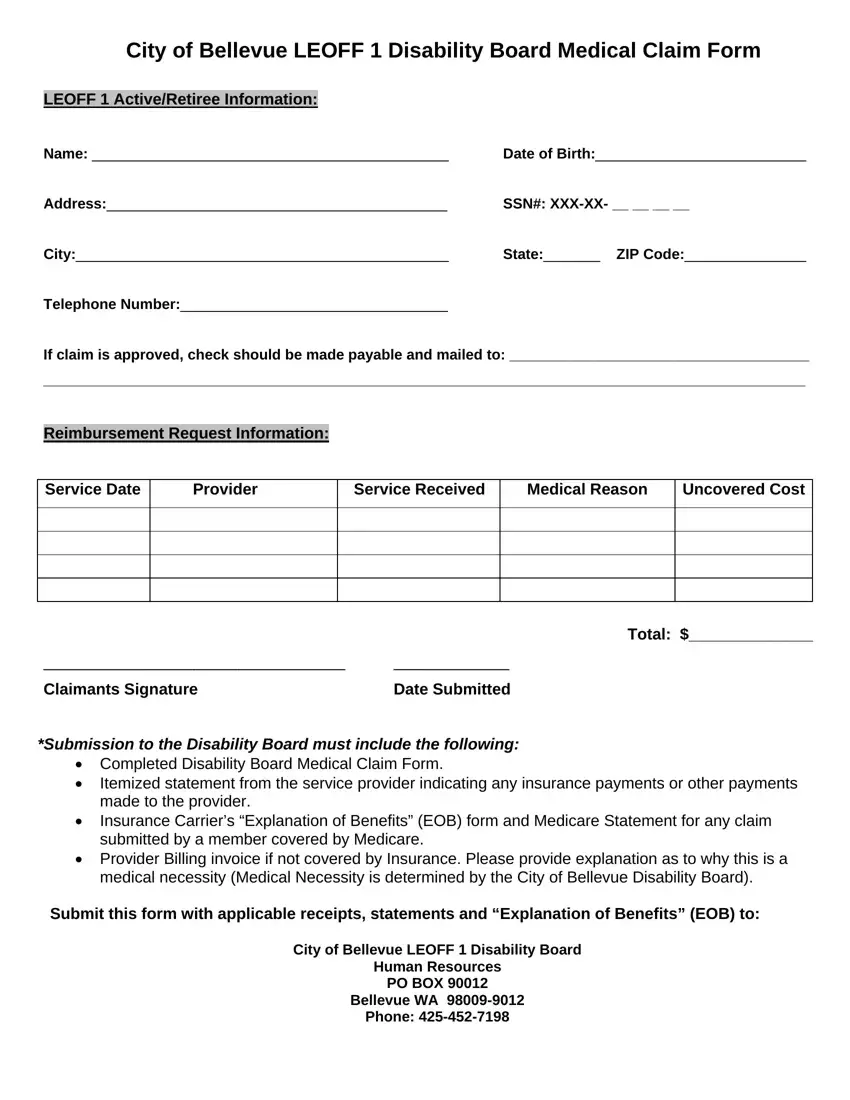
Please fill out the Claimants Signature, Date Submitted, Submission to the Disability Board, Total, Completed Disability Board, Itemized statement from the, Provider Billing invoice if not, and Submit this form with applicable field with the necessary data.
You will be asked for some valuable information if you want to complete the City of Bellevue LEOFF Disability, and HRetirement ServicesDisability section.

Step 3: Click "Done". Now you may export the PDF form.
Step 4: Attempt to create as many copies of your file as possible to prevent future issues.
