

What You Need Before Getting Started
Before opening the form in the editor, gather the following items to make the process faster and more accurate:
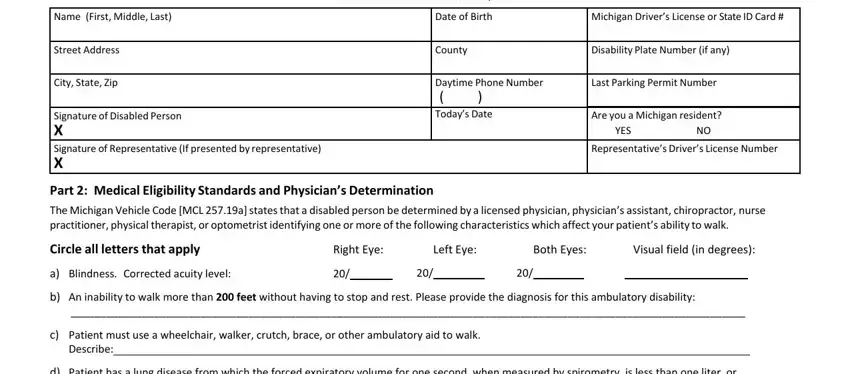
- Your full legal name, street address, city, state, and zip code
- Your date of birth and driver license or state ID number
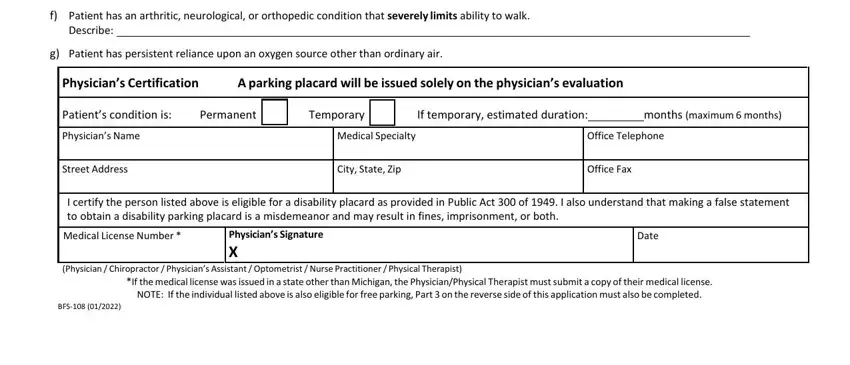
- Contact information for your certifying healthcare provider (physician, chiropractor, optometrist, nurse practitioner, or physician's assistant)
- The healthcare provider's office address, city, state, zip code, and office fax number
- A description of your qualifying mobility limitation and its expected duration
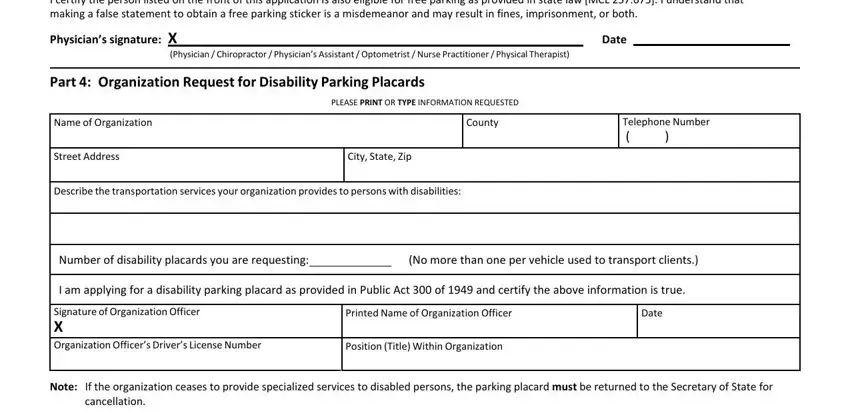
Organizations must also have the organization's name, county, telephone number, and the number of disability placards needed. If your provider needs a standardized form, the physician's statement for placard is available on FormsPal.
How to Fill Out the Application Using FormsPal
handicap parking permit michigan can be filled out easily. Simply try FormsPal PDF editor to perform the job quickly. To retain our tool on the leading edge of convenience, we aim to adopt user-driven features and enhancements regularly. We're at all times looking for feedback - play a pivotal part in reshaping PDF editing. To get the ball rolling, consider these easy steps:
Step 1: Click the orange "Get Form" button above. It'll open our pdf tool so you can begin completing your form.
Step 2: When you launch the editor, you will get the document made ready to be filled out. Apart from filling out various fields, you might also perform some other things with the PDF, specifically adding any text, modifying the initial text, inserting graphics, signing the form, and more.
This PDF form requires specific details to be filled out, hence make sure to take the time to type in what is requested:
1. The handicap parking permit michigan involves certain details to be entered. Be sure that the following blank fields are completed:
2. Soon after filling out the last step, go to the next stage and enter the necessary details in all these blank fields - patient incapable of meeting a, Describe, f Patient has an arthritic, Physicians Certification, A parking placard will be issued, Patients condition is, Permanent, Physicians Name, Street Address, Temporary, If temporary estimated duration, months maximum months, City State Zip, Office Fax, and I certify the person listed above.
3. In this particular step, look at that it almost completely impedes, I certify the person listed on the, Date, Physician Chiropractor , Part Organization Request for, Name of Organization, Street Address, City State Zip, Describe the transportation, PLEASE PRINT OR TYPE INFORMATION, County, Telephone Number , Number of disability placards you, No more than one per vehicle used, and I am applying for a disability. All these will need to be filled out with highest attention to detail.
You can certainly make an error when completing your Name of Organization, therefore you'll want to reread it before you'll finalize the form.
Step 3: Soon after going through your fields, hit "Done" and you're done and dusted! Get hold of the handicap parking permit michigan once you register at FormsPal for a 7-day free trial. Readily view the form within your FormsPal account, together with any modifications and adjustments being conveniently preserved! FormsPal provides safe form completion devoid of personal data record-keeping or any type of sharing. Feel comfortable knowing that your information is safe here!
After Submitting the Application
After submitting your completed disability parking placard application to a Michigan Secretary of State office, expect a standard processing time of 10 to 15 business days. You will receive your temporary or permanent disability parking placard by mail. Permanent placards require renewal every four years. Use the handicap placard renewal form on FormsPal when it is time to renew.
Common Questions About the Michigan Disability Parking Placard
Who can apply for a Michigan disability parking placard?
Any Michigan resident with a certified mobility-limiting disability may apply. Common qualifying conditions include inability to walk 200 feet without resting, need for an assistive device, severe cardiac or lung conditions, and significant orthopedic or neurological impairments. Organizations that regularly transport disabled persons may apply using Part 4 of the application.
Is there a fee to apply for a disability parking placard in Michigan?
No. There is no fee to obtain a disability parking placard. Qualifying residents may also benefit from free parking at metered spaces as allowed under Michigan law.
Can I complete this application online without printing first?
Yes. Use FormsPal's free PDF editor to fill in all required fields online, sign the document, download the completed PDF, and print it for submission at any Michigan Secretary of State branch office.
What is the difference between a temporary and permanent placard?
A temporary placard is issued when the healthcare provider determines the disability will last 3 to 12 months. A permanent placard is issued for long-term or permanent conditions. Both require a completed application form and a signed medical certification from a licensed provider.