We were developing our PDF editor with the idea of making it as effortless to use as possible. That's why the actual procedure of creating the bwc c84 form will likely to be easy carry out these steps:
Step 1: Look for the button "Get Form Here" on the website and press it.
Step 2: Now, you are on the form editing page. You may add information, edit existing details, highlight specific words or phrases, put crosses or checks, add images, sign the file, erase unneeded fields, etc.
If you want to fill in the bwc c84 form PDF, provide the details for each of the sections:
Provide the necessary particulars in the Where do I file the C, For injured workers whose employer, For all other injured workers You, Where do I find more information, For injured workers whose employer, For all other injured workers, You can obtain BWC forms at, and C BWC Rev March area.
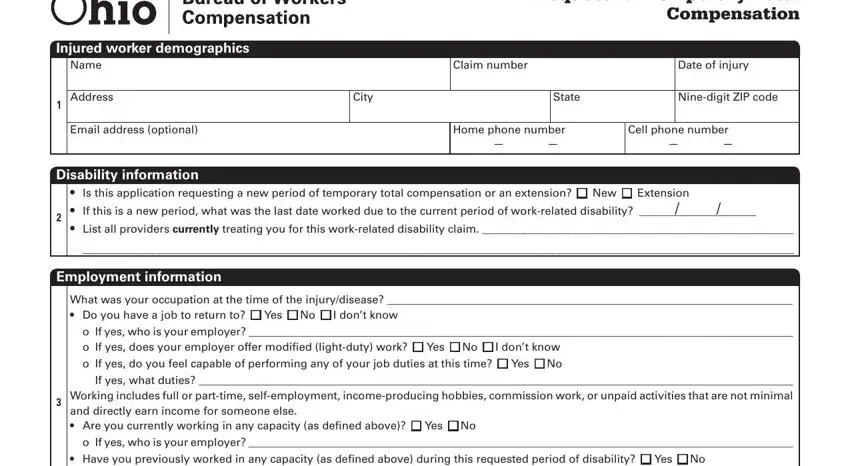
Within the area referring to Injured worker demographics, Name, Address, Email address optional, Disability information, Request for Temporary Total, Claim number, Date of injury, City, State, Ninedigit ZIP code, Home phone number, Cell phone number, Is this application requesting a, and Employment information, it's essential to note down some required information.
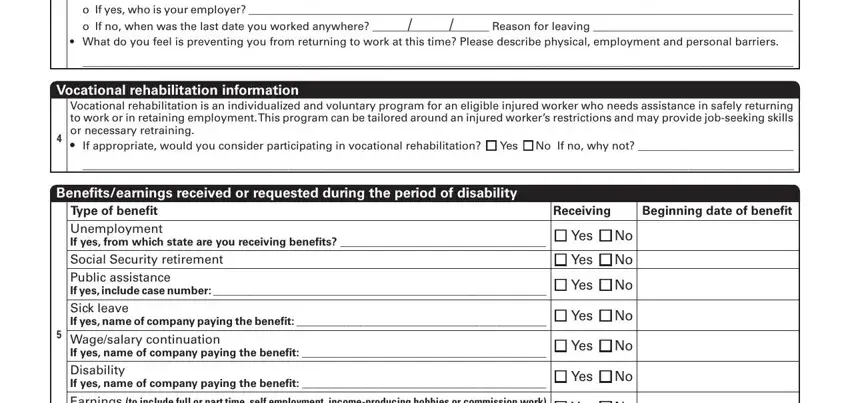
Inside the section o If yes who is your employer o, Vocational rehabilitation, Vocational rehabilitation is an, Benefitsearnings received or, Receiving Beginning date of benefit, Type of benefit Unemployment If, n Yes n No, n Yes n No, n Yes n No, n Yes n No, Wagesalary continuation If yes, n Yes n No, n Yes n No, Earnings to include full or part, and n Yes n No, list the rights and responsibilities of the parties.
Finalize by reading all of these fields and filling out the required information: Earnings to include full or part, n Yes n No, Injured worker signature, I understand I am not permitted to, Date, and C BWC Rev March.
Step 3: Select the "Done" button. Now you can export your PDF document to your electronic device. Additionally, you may forward it by electronic mail.
Step 4: Be certain to avoid potential complications by generating no less than 2 duplicates of the file.
