 Yes
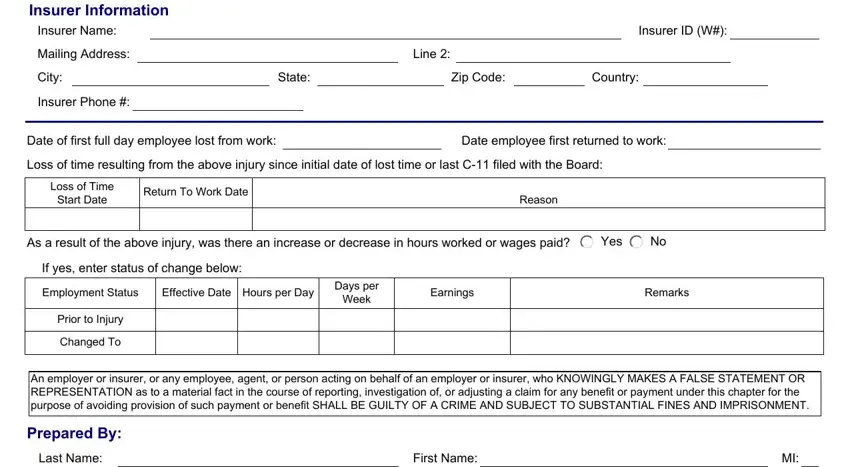
Yes  No If yes, enter status of change below:
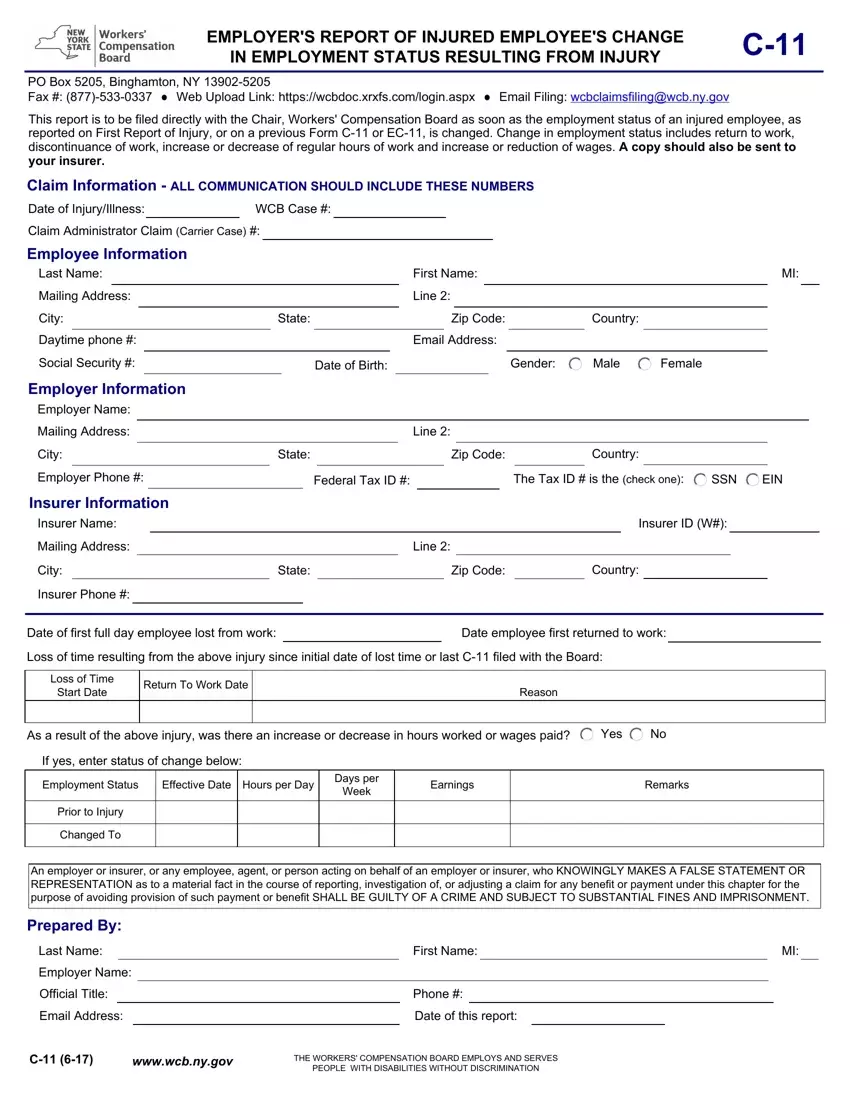
No If yes, enter status of change below:Filling in the c 11 form nys form is easy using our PDF editor. Follow these steps to create the document right away.
Step 1: Select the button "Get Form Here" on this webpage and next, click it.
Step 2: Once you access the c 11 form nys editing page, you'll see lots of the options it is possible to undertake with regards to your form in the top menu.
For each section, complete the content requested by the application.
Write down the necessary data in Insurer Information, Insurer Name, Mailing Address, City, Insurer Phone, Line, State, Zip Code, Country, Insurer ID W, Date of first full day employee, Date employee first returned to, Loss of time resulting from the, Loss of Time Start Date, and Return To Work Date box.
Describe the significant particulars in the Employer Name, Official Title, Email Address, Phone, Date of this report, wwwwcbnygov, and THE WORKERS COMPENSATION BOARD part.

Step 3: Hit the Done button to save the form. Now it is accessible for upload to your electronic device.
Step 4: In order to prevent probable future difficulties, take the time to obtain up to a few copies of each document.
