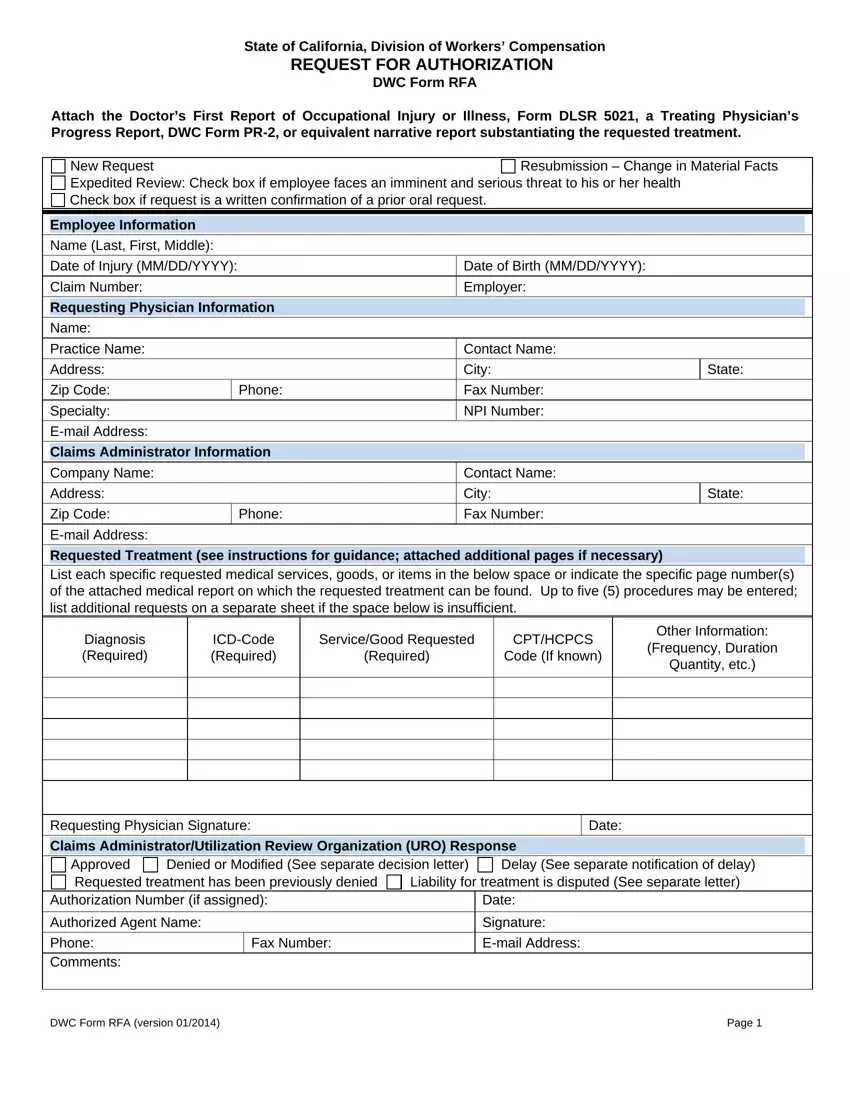
The State of California, Division of Workers’ Compensation, plays a critical role in ensuring employees receive necessary medical treatment for occupational injuries or illnesses through the Request for Authorization (RFA) form, officially known as DWC Form RFA. This essential document facilitates the utilization review process, as mandated by Labor Code section 4610, by allowing treating physicians to request authorization for proposed treatments. To substantiate the need for the requested treatment, it must be accompanied by relevant medical reports such as the Doctor’s First Report of Occupational Injury or Illness, Form DLSR 5021, a Treating Physician’s Progress Report, DWC Form PR-2, or an equivalent narrative report. The form accommodates a range of requests, from new treatment applications to resubmissions due to changes in the patient's condition. Additionally, provisions are made for expedited reviews in situations posing imminent and serious health threats to the employee, along with the procedure for submitting a written confirmation of prior oral requests. The form systematically captures detailed employee information, specifics of the requested treatment, and the physician’s diagnosis, relying on ICD and CPT/HCPCS codes to clarify needs. It further outlines the expected response from the claims administrator or Utilization Review Organization (URO), ensuring a streamlined process for approving, denying, or modifying the requests. This structured approach not only protects sensitive healthcare information but also underscores the comprehensive measures in place to support workers’ health and well-being in California.
| Question | Answer |
|---|---|
| Form Name | Ca Form Rfa |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | printable rfa form, ca dwc rfa, workers comp rfa form pdf, dwc form rfa fillable |
