We were designing our PDF editor with the prospect of making it as quick make use of as possible. For this reason the procedure of filling out the wcb ny onlinb form rfa 1w will be simple as you go through the next actions:
Step 1: To begin the process, select the orange button "Get Form Now".
Step 2: You will find each of the actions that you may use on the template once you have accessed the wcb ny onlinb form rfa 1w editing page.
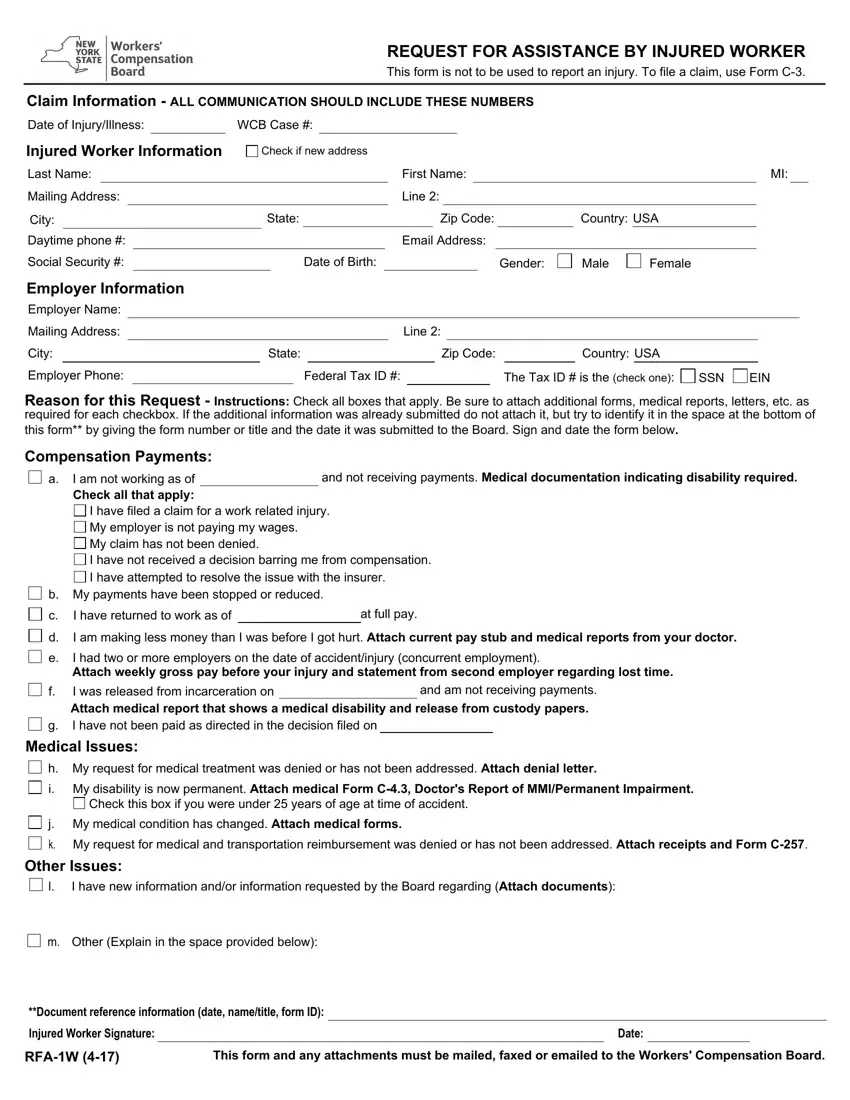
Please enter the next details to prepare the wcb ny onlinb form rfa 1w PDF:

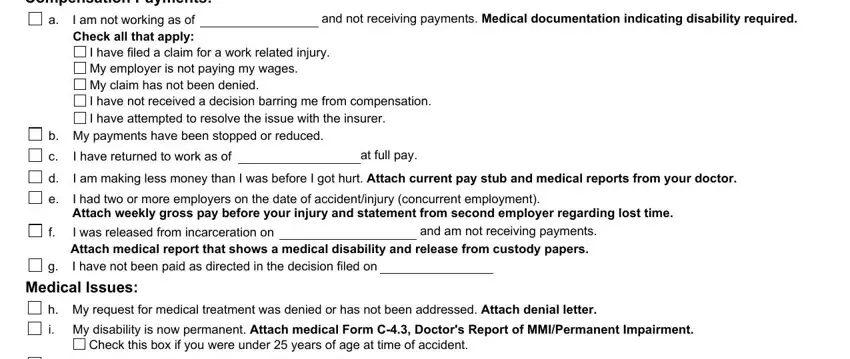
Type in the necessary particulars in Compensation Payments, I am not working as of Check all, and not receiving payments Medical, I have filed a claim for a work, b My payments have been stopped or, I have returned to work as of, at full pay, I am making less money than I was, I had two or more employers on the, and am not receiving payments, Medical Issues, h My request for medical treatment, i My disability is now permanent, and Check this box if you were under box.
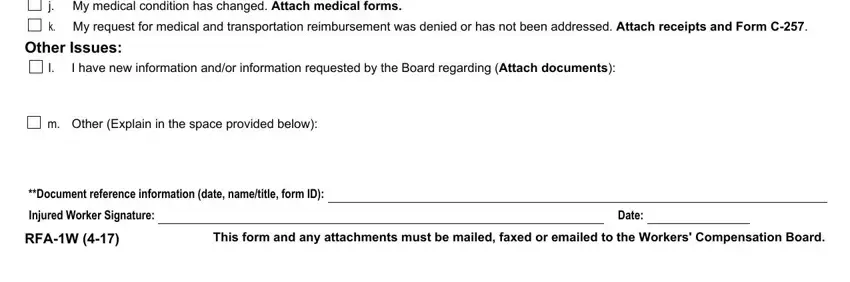
Type in all information you are required inside the section j My medical condition has changed, k My request for medical and, Other Issues, I have new information andor, m Other Explain in the space, Document reference information, Injured Worker Signature, RFAW, This form and any attachments must, and Date.
Step 3: Choose the Done button to be certain that your finalized file may be transferred to any type of device you want or mailed to an email you specify.
Step 4: Create at least two or three copies of your document to avoid all of the potential future concerns.
