
Who Needs the California ACP Form?
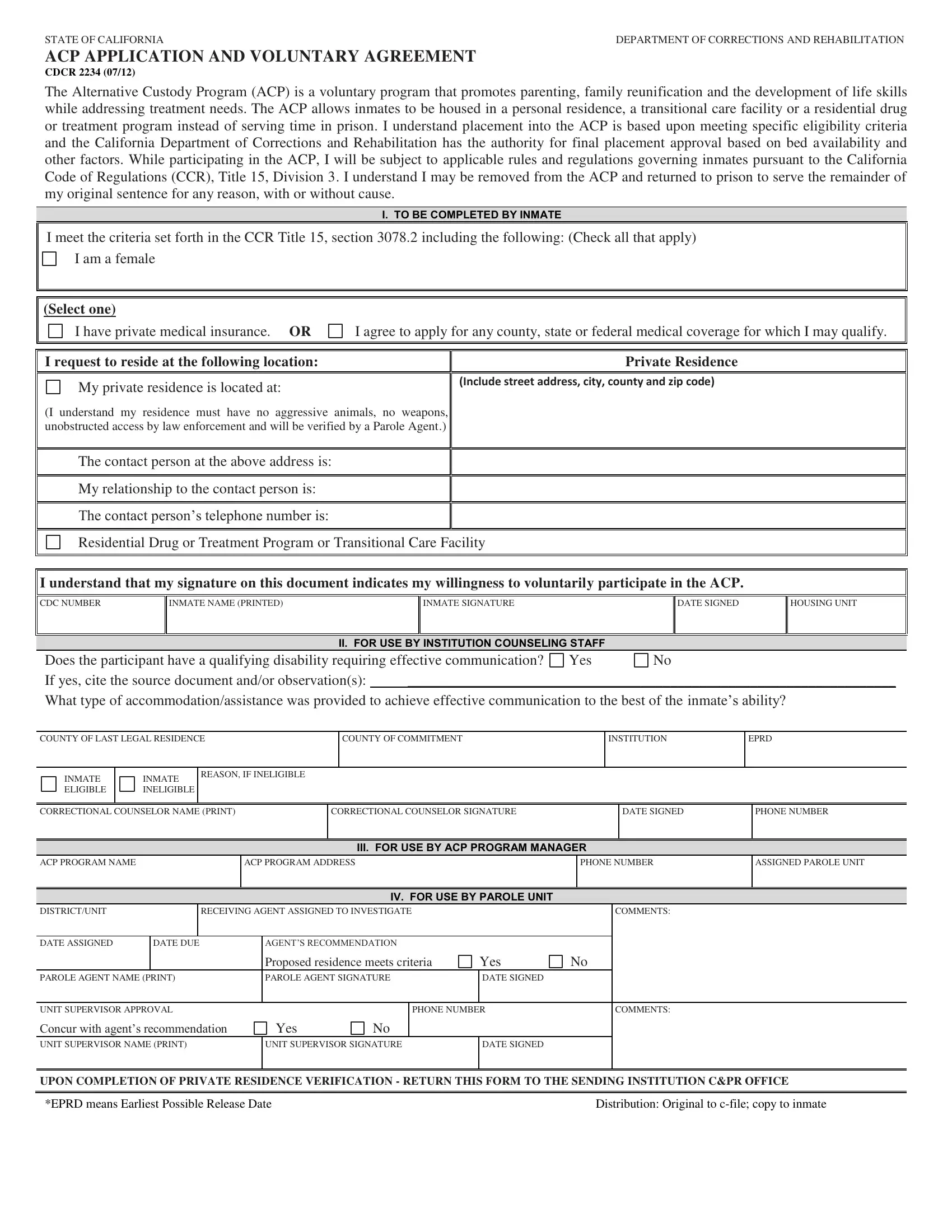
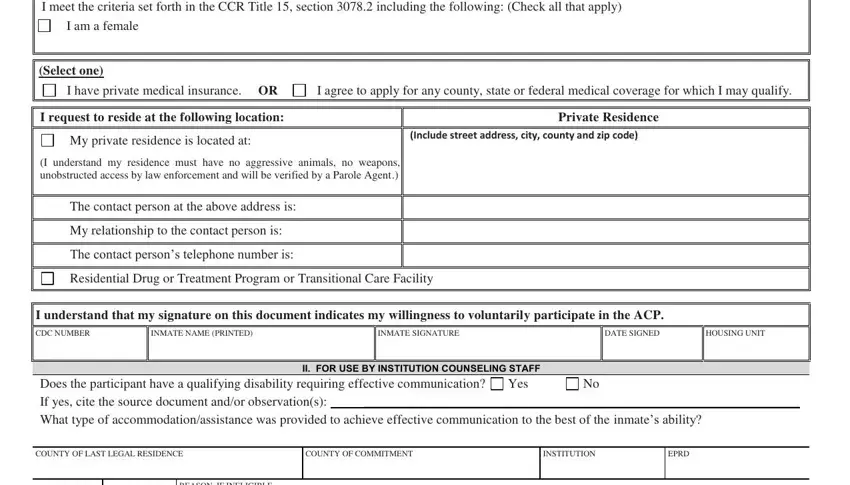
The California Alternative Custody Program application form is needed by inmates applying for ACP placement. It is also used by correctional counselors, legal representatives, and family members assisting with the application. Anyone who wants to participate in the program must complete and submit Form CDCR 2234 to the CDCR for review.
How to Fill Out the CDCR ACP Application Online
Completing this form online is straightforward using our PDF editor. Follow the steps below to get started.
Step 1: Click the "Get Form" button at the top of this page to open the PDF editor. The editor loads all the tools you need to complete your document.
Step 2: Use the editor to fill in the form fields, add text, and make any needed corrections. You can also add graphics and sign the form within the editor.
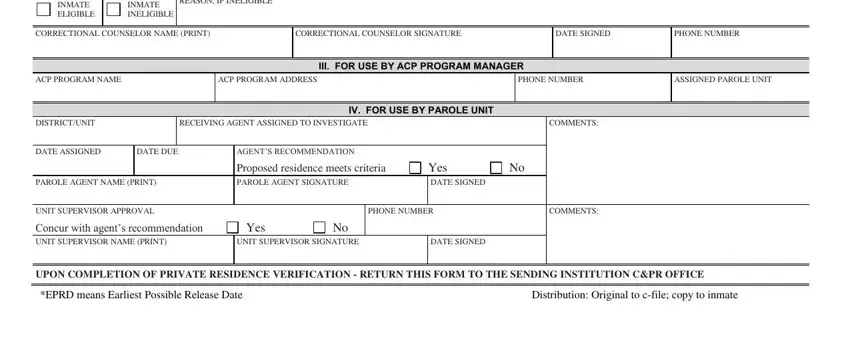
Step 3: Complete all required fields in the form. Pay close attention to each blank to avoid errors. The form includes fields such as INMATE ELIGIBLE, INMATE INELIGIBLE, REASON IF INELIGIBLE, CORRECTIONAL COUNSELOR NAME, CORRECTIONAL COUNSELOR SIGNATURE, DATE SIGNED, PHONE NUMBER, ACP PROGRAM NAME, ACP PROGRAM ADDRESS, ASSIGNED PAROLE UNIT, RECEIVING AGENT, and COMMENTS.
Step 4: Review all completed fields before submitting. Check the DATE SIGNED field carefully. Mistakes in this field are common. Once you are satisfied with the form, click "Done" to save your work.
Step 5: Download the completed CDCR ACP application as a PDF. You can also send it by email directly from the editor. All saved documents appear in your account for easy access later.
Frequently Asked Questions
What is the California Alternative Custody Program?
The California ACP is a voluntary program run by the CDCR. It allows eligible inmates to serve their sentences in approved community settings instead of prison. Approved settings include private homes, transitional care facilities, and residential treatment programs.
Who is the ACP designed for?
The program is designed primarily for female inmates who are primary caregivers for minor children. Applicants must meet custody classification requirements and must not have convictions for certain violent offenses.
How does the ACP application process work?
An inmate submits Form CDCR 2234 to their correctional counselor. The counselor reviews eligibility and forwards the application to the ACP program manager. The CDCR then evaluates the application and makes a placement decision. The process can take several weeks depending on the complexity of the case.
What happens if someone violates ACP program rules?
Violating program rules results in removal from the ACP. The participant is returned to prison to complete the remainder of their original sentence. There is no automatic right to return to the program after a removal.
Is the CDCR 2234 form the same as the california alternative custody application?
Yes. Form CDCR 2234 (07/12) is the official name for the California Alternative Custody Program Application and Voluntary Agreement. Some documents refer to it simply as the ACP application or the cdcr acp application form.
Related California Legal Forms
You may also need these related documents when working with California custody and corrections paperwork.
- Temporary Custody Form
- Documentation Proof of Incarceration
- County Community Supervision and Corrections Form
- Non-Incarceration Status Form
FormsPal stores all your documents safely. Your personal data is never shared or recorded. Complete your california alternative custody form with confidence.